
2024-108 Alameda County Department of Children and Family Services
Delayed Investigations and Support Services Risk the Health and Safety of Youth
Published: September 23, 2025Report Number: 2024-108
September 23, 2025
2024‑108
The Governor of California
President pro Tempore of the Senate
Speaker of the Assembly
State Capitol
Sacramento, California 95814
Dear Governor and Legislative Leaders:
As directed by the Joint Legislative Audit Committee, my office conducted an audit of the Alameda County Department of Children and Family Services (department) regarding its role in ensuring the health and safety of youth in the county’s foster care system. In general, we determined that the department did not always initiate investigations of alleged child abuse and neglect referrals within the prescribed time frames, did not always ensure that foster youth received timely critical physical and mental health services, and did not always ensure that youth maintained connection with family members.
The department must initiate investigations within one day when youth are in imminent risk (immediate referrals) and within 10 days when youth are not at imminent risk (non‑immediate referrals); however, the late initiation of such investigations has increased since fiscal year 2019–20. In fiscal year 2023–24, the department initiated investigations of 11 percent of immediate referrals and 48 percent of non‑immediate referrals after the required time frames. Furthermore, the department did not complete investigations within the prescribed 30 days after initiation, and it took the department an average of 105 days to complete investigations for about half of all non‑immediate referrals in fiscal year 2023–24. Although delays in initiating investigations of the referrals that we selected for review were beyond the department’s control—when, for example, the department was unable to contact a family member after repeated attempts—the department could not always demonstrate why its completion of investigations took so long. We acknowledge that the department has faced high job vacancies, which has resulted in large caseloads for its staff in the Emergency Response Unit—the unit responsible for conducting investigations.
Because it lacked necessary documentation, the department could not demonstrate or did not ensure that youth received needed services in a timely manner. Inconsistent documentation leaves the department unable to know whether its staff have made adequate efforts to ensure that youth receive services in a timely manner. Similarly, we found that the department’s documentation did not include information about its efforts to identify, locate, and notify all relatives who could serve as potential caretakers or to engage youth with family members to expand the youths’ potential support networks.
Without timely investigations and thorough documentation, the department runs the risk of leaving youth in potentially unsafe circumstances or of not providing vital services that youth in its care require for their well‑being, family connections, and successful transition into adulthood.
Respectfully submitted,
GRANT PARKS
California State Auditor
Selected Abbreviations Used in This Report
| CCWIP | California Child Welfare Indicator Project |
| CDSS | California Department of Social Services |
| CFE | Center for Excellence |
| CFT | Child and Family Team |
| CHDP | Child Health and Disability Prevention |
| ER Unit | Emergency Response Unit |
| IEP | Individualized Education Plan |
| ILT | Interagency leadership team |
| IPP | Individual Program Plan |
| MOU | Memorandum of Understanding |
| RBA | Results‑based accountability |
| SDM | Structured decision making |
| STRTP | Short Term Residential Therapeutic Placement |
| WCCC | WestCoast Children’s Clinic |
Summary
Key Findings and Recommendations
The Alameda County Department of Children and Family Services (department) is responsible for protecting the more than 300,000 youth who live in the county by providing child abuse and neglect prevention services, responding to child abuse and neglect reports, and providing needed services to youth in the foster care system. From fiscal years 2019–20 through 2023–24, the department received nearly 57,000 reports of alleged child abuse and neglect. When the department receives a report of alleged child abuse and neglect through its centralized hotline, an intake worker may initiate a referral for investigation. If the referral indicates that youth are in imminent danger of physical pain, injury, disability, severe emotional harm, or death (immediate referral), the department must conduct an in‑person investigation within 24 hours of receiving the referral. When an allegation could constitute abuse or neglect, but the youth is not at imminent risk (non‑immediate referral), state law requires an in‑person investigation within 10 days. A child welfare worker then performs an investigation to evaluate the risk of the youth’s safety and assesses the possible need for out‑of‑home placement. In our review of the timeliness of investigations of alleged child abuse and neglect referrals and the provision of services to foster youth, we found that the department did not initiate about half of its investigations within the prescribed time frames, did not ensure that foster youth received timely critical physical and mental health services, and did not adequately report critical incidents that occurred at its Transitional Shelter Care Facility (transitional shelter). Until the department addresses these significant shortcomings, it cannot ensure that it is taking sufficient action to address the health and safety needs of Alameda County’s youth.
High Job Vacancy Rates and Caseloads Have Contributed to Delays in Investigations of Alleged Child Abuse and Neglect
From fiscal years 2019–20 through 2023–24, the department did not consistently initiate or complete investigations of child abuse and neglect referrals within the required time frames, leaving youth in potentially unsafe situations. The department initiated investigations after the prescribed 24‑hour time frame for 5 percent to 11 percent of the more than 1,000 immediate investigation referrals per year from fiscal years 2019–20 through 2023–24, and initiated investigations after the prescribed 10‑day time frame for 17 percent to 49 percent of about 2,000 non‑immediate investigation referrals per year during the same period. For example, in fiscal year 2022–23, the department initiated investigations of 1,030, or 49 percent, of the non‑immediate referrals after 10 days, while the average number of days to initiate these late investigations was 187 days. We also found that after initiating investigations, the department did not always complete them within the required time frames. For the referrals it investigated, the department closed investigations of between 51 and 59 percent of immediate referrals per year and between 59 and 75 percent of non‑immediate referrals per year after the prescribed 30‑day time frame. We found that fiscal year 2021–22 had the longest average number of days to close late investigations with the department closing investigations of about 1,000 immediate referrals in 407 days, on average.
The department attributed the delays to its child welfare worker vacancy rates and high caseloads. The department also noted that the intense and often traumatic nature of the work, with exposure to challenging situations involving youth and families, can lead to stress and burnout among child welfare workers. The department’s child welfare workers whom we interviewed, and the responses to a department survey of employees completed in 2023, also identified stress as one of the most significant challenges child welfare workers face. Our review showed that from fiscal years 2019–20 through 2024–25, the department’s vacancy rates doubled from 17 percent to 34 percent for child welfare workers and more than doubled from 8 percent to about 18 percent for supervisors. The many vacancies in Alameda County have resulted in child welfare workers at the department’s Emergency Response (ER) Unit having caseloads higher than the guideline that recommends 15 new cases per month. The ER Unit plays a critical role as it is responsible for investigations of immediate referrals. These vacancies have reduced the department’s ability to meet the needs of the county’s youth and families. Even though the department has implemented some strategies to address its vacancies—such as using involuntary staff transfers to help address open referrals and reduce caseloads in its ER Unit—we believe that the department could hire more child welfare workers in its ER Unit in the Child Welfare Worker I position, which only requires the individual to have earned a bachelor’s degree. It could also implement a mandatory practice that new staff shadow more experienced child welfare workers to reduce the time supervisors spend training new staff.
The Department Has Not Ensured That Interagency Partners Provide Timely Services, Risking the Health and Safety of Foster Youth
To provide foster youth with coordinated and trauma‑informed services, Alameda County established a Memorandum of Understanding (MOU) in May 2022 with public and private partners, including the Alameda County Behavioral Health Department, the Alameda County Office of Education, the Regional Center of the East Bay, and the Alameda County Probation Department. The MOU directs these interagency partners to provide youth with certain services, such as educational, developmental, and mental and behavioral health services, and it requires the partners to coordinate referrals, screening, eligibility, and authorization of therapeutic care for youth with complex emotional and behavioral needs. The department could not ensure that youth received needed services in a timely manner because it did not consistently document and track the frequency and the timeliness of services provided by its interagency partners or the department’s contractors. To determine whether the department provided timely services, either directly or through its interagency partners, we reviewed 36 case files in which youth were referred to 125 specific services. Sixty‑five of these 125 referred services lacked the necessary documentation, such as treatment summaries and detailed notes about when services were provided, to determine whether the youth received timely services. Although child welfare workers generally made their monthly visits to foster youth as required, existing contact notes from those visits included inconsistent or inadequate details about the frequency and dates of services youth received. For example, for six of the 10 sexual health education services we reviewed, the department lacked sufficient documentation to demonstrate when the youth received the service.
Additionally, when we could evaluate timeliness, the services were delayed from an average of three months for health services to more than a year for sexual health education services. For example, youth should receive health and dental services within 30 days of a court’s determination to remove youth from the home. Of the 28 health services that we reviewed for timeliness, 11 were delayed by an average of 85 days after the 30‑day time frame. Although the causes of most of the delays appear to be circumstances outside of the department’s direct control—such as delays in families’ receiving Medi‑Cal cards and youth who were absent from their respective placement without permission—inconsistent documentation leaves the department unable to know whether staff have made adequate efforts to ensure that youth receive services in a timely manner. Finally, the department’s MOU does not require partner agencies to provide necessary documentation of services to be provided and when they were actually provided. Insufficient documentation leaves the department without the information necessary to ensure that the terms of its MOU are appropriate for accomplishing the goal of a coordinated, integrated, and effective delivery of services for children, youth, and families.
The Department’s Efforts to Connect Youth With Family and Keep Them Safe in Temporary Shelter Have Been Inadequate
The department did not prioritize efforts to ensure that foster youth had ongoing connections with family members. When a court orders the removal of a youth from the custody of their caretaker for reasons necessary to protect the youth, the department should, within 30 days, conduct an investigation to identify, locate, and notify all relatives of their option to provide support or possible placement for the foster youth with the relative. The department reports to the court every six months on the status of the case, which should also include a discussion about the department’s efforts to enhance the youth’s family connections. In all five cases we reviewed, we found that the department’s report to the court did not include information about the efforts the department took, such as asking the youth about their relatives and contacting all identified relatives by telephone, email, or through in‑person visits, to identify, locate, and notify all relatives who could serve as potential caretakers. We also found that the department did not perform continued efforts to engage youth with family members to expand the youth’s potential support networks (family finding and engagement).
The department operated a transitional shelter until July 2024. The California Department of Social Services (CDSS) allowed the department to house at this transitional shelter, for up to 72 hours, youth who did not have immediate placement options and were awaiting stable placement. However, youth at this transitional shelter may have faced risks, including assaults and drug use, while they were at the facility or away from the transitional shelter without authorization (missing from care). The transitional shelter cannot force youth to stay in the shelter and some of the youth may leave the transitional center at their own discretion and go missing from care. Our review of 166 critical incidents—such as injuries that require medical attention or those in which youth were missing from care—that the department reported to CDSS from August 2020 through July 2024 found that the most prevalent critical incidents included those in which a youth threatened to assault another youth or staff members. Further, our review of critical incident reports found that youth who were missing from care were often involved in critical incidents that included drug or alcohol use. Further, CDSS’s inspection reports from fiscal years 2020–21 through 2023–24 identified deficiencies related to the department’s reporting of critical incidents.
Other Areas We Reviewed
In addition, we reviewed the department’s compliance with training requirements for child welfare workers and supervisors. From fiscal years 2019–20 through 2023–24, many department staff did not complete the required training, citing issues of workload, scheduling conflicts, and staff absences. We also reviewed the department’s contracts with providers of services for youth to determine whether the contracts provided time frames for service delivery or performance metrics for timely delivery of services, and we found that most contracts did not include such metrics for timeliness. Without the timeliness metrics, the department may not be able to track whether its contractors provide service within the agreed upon time frames. However, the department agreed that having performance metrics for timeliness in its contracts would ensure better provision of services to foster youth.
To address these findings, we have made recommendations to the department that it should periodically review the status of all referrals to determine the number of days to initiate and complete investigations and work with staff to identify any impediments. In doing so, we recommended that it should develop a strategy to address all identified impediments to ensure that it reduces the number of days for initiating and completing all investigations to comply with required time frames. Further, we recommended that it should track the timeliness of support services, including whether youth have or have not received needed services, and it should ensure that its contracts include timeliness metrics.
Agency Comments
The department agreed with our recommendations and indicated that it will implement them.
Introduction
Background
State law affords youth1 who are placed in the foster care system various rights. Among such rights are the right to live in a safe, healthy, and comfortable home where they are treated with respect; the right to be free from physical, sexual, emotional, or other abuse; and the right to be free from corporal punishment and exploitation. To further the intent that all children are safe and free from abuse and neglect, state law mandated the creation of a public system of statewide child welfare services through CDSS and county welfare departments. Specifically, CDSS is responsible for providing oversight and guidance to counties. Counties are responsible for investigating reports of neglect and abuse, and taking steps to protect youth, including removing youth from their homes and placing them in the foster care system. In Alameda County, which is home to about 330,000 youth, its Social Services Agency is responsible for administering public social services in providing aid and services to families with dependent youth in Alameda County. As of July 2024, approximately 700 of those youth were in foster care.2
California Department of Social Services
State law requires CDSS to review child welfare services throughout the State. CDSS develops and oversees programs and services for at‑risk youth and families, as the text box shows, and it provides detailed guidance that counties must use to make decisions regarding child welfare services. One element of CDSS’s guidance is its provision to county welfare departments of Structured Decision Making (SDM) tools for screening reports of alleged child abuse and neglect and evaluating the safety risks for alleged victims who are the subjects of such reports.
California’s Child Welfare Services Include Programs and Services Intended to Do
the Following:
- Prevent abuse or strengthen families.
- Remedy the effects of abuse and neglect, through emergency response and family maintenance and family reunification.
- Provide for the out‑of‑home care of children, such as foster care and relative home placements.
- Provide for the permanent removal of children from abusive homes, through adoptions, legal guardianship, and kinship care.
Source: CDSS.
In 1989, state law authorized the development of the child welfare services case management system (CWS/CMS), which now links the State’s 58 counties and CDSS to a common online database that tracks each case from initial contact through termination of services. Counties and the State use CWS/CMS for all case management, service planning, and information gathering functions of child welfare services.
Alameda County Department of Children and Family Services
The Department of Children and Family Services (department) within the Alameda County Social Services Agency organizes and operates its own programs for child welfare services. With the direction of state law, the department is responsible for responding to reports of alleged child abuse and neglect and providing needed services to youth in the foster care system. To fulfill these responsibilities, the department determines whether a youth can safely remain in the home or should be removed from the home and which of the department’s several programs—such as family maintenance, family reunification, or permanency planning, as Figure 1 shows—will best support the youth.
Figure 1
The Department’s Approach to Determining Whether a Youth Can Safely Remain at Home or Should Be Removed
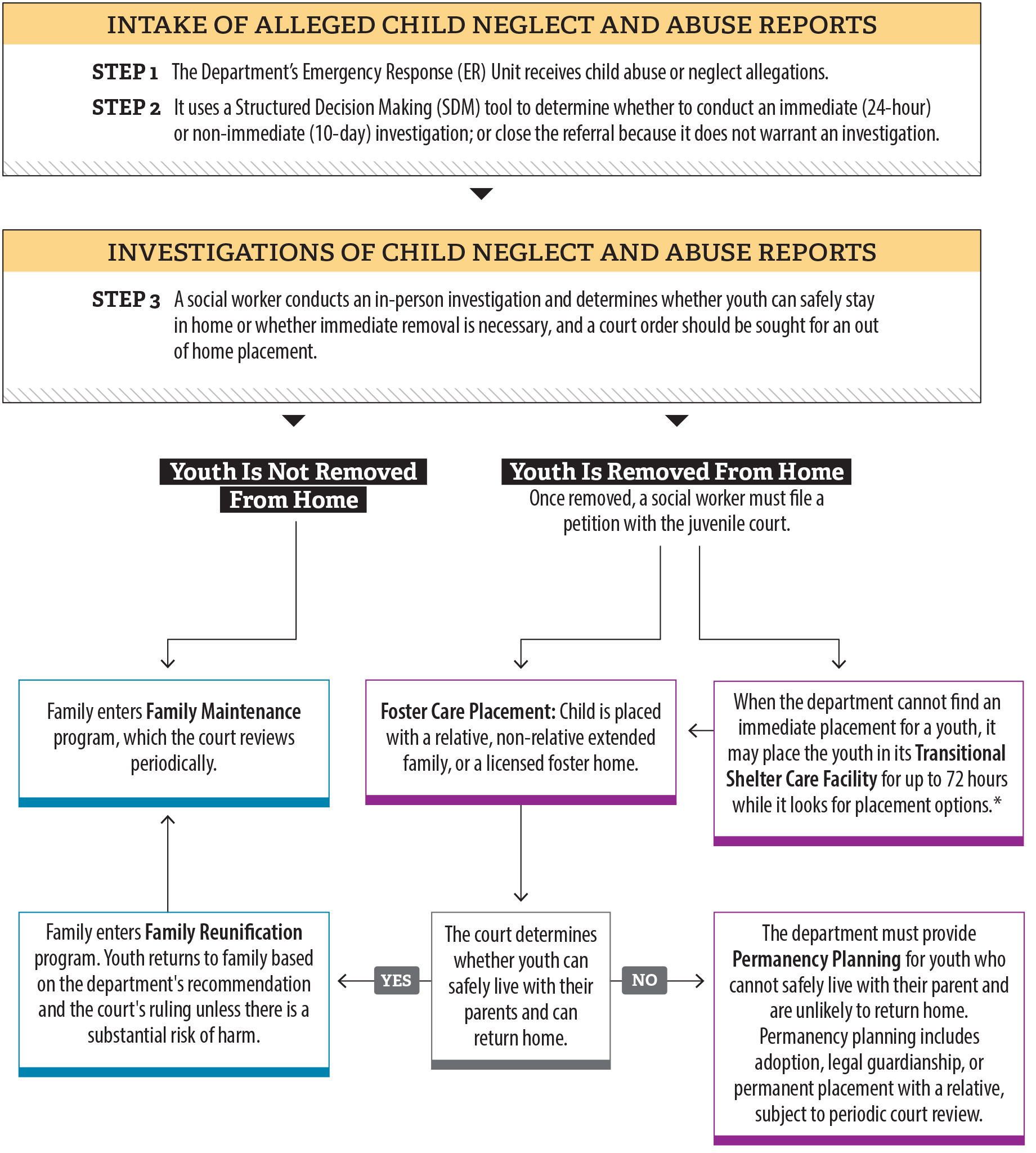
Source: State law, CDSS’s Child Welfare Services Manual, and the department’s Juvenile Dependency Flow Chart.
Note: The service components are simplified to show areas relevant to the audit subject. The department may have other services that are not represented in the graphic.
* Until July 2024, in cases where the department could not find an immediate suitable placement for youth, the department had the option to temporarily place youth in its transitional shelter. The department plans to reopen the shelter at a new location.
Figure 1 is a color-coded flow chart that describes the steps in receiving and investigating reports of alleged child neglect and abuse. The first box describes the two steps involved in intake of alleged child neglect and abuse reports. The next box indicates how the department investigates referrals. Next, the flow chart describes that when a youth is not removed from the home, the family enters a family maintenance program, which is reviewed every six months. The flow chart also shows that when a youth is removed from the home, the youth can be placed with a foster family or in a transitional shelter care facility for up to 72 hours, if immediate placement is not found. The court then determines if youth can safely live with their parents and return home. If so, the family enters Family Reunification program and then enters family maintenance, which the court reviews periodically. Otherwise, the department must provide Permanency Planning, which includes adoption, legal guardianship, or permanent placement with a relative, subject to periodic court review.
State law requires the department to provide family maintenance services to families whose children have become dependents of the court because of neglect, abuse, or other circumstances that create a substantial risk that the child may suffer serious physical harm or illness. The department provides family maintenance services, such as parenting courses in handling anger or child development, therapies, and other services to help maintain youth safely in their homes. If a child welfare worker decides to separate youth from their parents because of abuse and neglect, the department provides family reunification services with the purpose of reuniting youth with their parents. For youth who cannot safely live with their parents and are not likely to return to their homes, the department arranges permanency planning, allowing child welfare workers to seek adoption for the youth and terminate reunification services.
Reports of Alleged Child Abuse and Neglect
From fiscal years 2019–20 through 2023–24, the department received nearly 57,000 reports of alleged child abuse and neglect. State law requires the department to operate a 24‑hour emergency response system to receive and respond to reports of alleged child abuse and neglect. When individuals suspect child abuse or neglect, they can report it directly to the department through its 24‑hour emergency hotline. Furthermore, state law mandates that individuals in certain professions or roles that frequently interact with youth—such as teachers, physicians, counselors, or athletic coaches, and those who are referred to as mandated reporters—report all suspected child abuse and neglect. Examples of child abuse and neglect allegations include willfully harming or injuring a child, general neglect, sexual assault, or other allegations that the text box describes. After the department receives a report of an allegation, an intake worker may open a referral for either an immediate or non‑immediate investigation or may close it if the report does not warrant an investigation.
Child Abuse and Neglect Allegations Reportable to the Department Include:
Willfully Harming or Injuring a Child or Endangering the Health of a Child: When any person willfully causes or permits any child to suffer, or inflict thereon, unjustifiable physical pain or mental suffering or when a person with the custody of a child willfully causes or permits the health of a child to be endangered.
Unlawful Corporal Punishment: When any person willfully inflicts upon any child cruel or inhumane corporal punishment or injury resulting in a traumatic condition.
Sexual Abuse: Sexual assault and sexual exploitation.
Severe Neglect: Failure of a caretaker to protect a child from severe malnutrition or medically diagnosed nonorganic failure to thrive, or willfully placing the child’s health or safety at risk by intentional failure to provide adequate food, clothing, shelter, or medical care. General Neglect: Failure of a person with custody of a child to provide adequate food, clothing, shelter, or medical care or supervision where the child is at risk of suffering serious physical harm or illness.
Source: State Law.
Referrals and Investigations
There are three different outcomes a referral to investigate child abuse or neglect can produce, as the text box shows. When referrals indicate that youth are in imminent danger, the department must conduct an immediate in‑person investigation within 24 hours. If an allegation could constitute abuse or neglect but the youth is not at imminent risk, state law requires an in‑person response within 10 calendar days. For context, in each of the last six years, fiscal years 2019–20 through 2024–25, the department received reports of between 1,000 and 1,700 child abuse and neglect allegations that required immediate investigation, and it received between 1,500 and 2,100 for non‑immediate investigation. During an investigation, a child welfare worker interviews the youth and other parties involved in referrals to determine what actions, if any, are necessary to protect the youth from further abuse. When investigations substantiate the allegation, meaning the investigation determines that the alleged abuse or neglect more likely than not occurred, the department uses CDSS‑prescribed SDM tools3 to determine the next steps, including whether the youth can remain safely at home or should be removed from the home.
Possible Outcomes of Referrals of Child Abuse and Neglect
Unfounded investigation: The department’s investigation determines that the alleged abuse or neglect was false, was inherently improbable, involved an accidental injury, or did not constitute child abuse or neglect.
Inconclusive or unsubstantiated investigation: Because of a lack of sufficient evidence, the department could not determine whether the allegations of abuse or neglect occurred.
Substantiated investigation: The department’s investigation determines that the alleged abuse or neglect more likely than not occurred.
Source: State law and CDSS Child Welfare Services Program Requirements.
Structured Decision Making
The department assesses a youth’s immediate safety and the risk of future maltreatment using SDM tools. The SDM tools aid child welfare workers in determining the response priority required for reported incidents of child abuse and neglect. For example, the SDM tools help intake workers determine whether an in‑person investigation is warranted by answering specific questions the tools ask about the type of allegation, location of allegation, and historical information about the alleged victim and perpetrator. After a child welfare worker initiates an investigation, the SDM tools also assist the worker in making safety assessments to measure the presence of immediate safety threats in the home and risk assessments to determine the likelihood of future maltreatment and future child welfare system involvement.
Youth Placement Decisions
Before taking a youth into its custody, state law requires the department to consider whether a youth may remain safely in the home. If the department finds that taking the youth into custody is necessary for the youth’s health and safety, and the youth is not released to a parent or guardian, the department must petition a juvenile court to declare the youth a dependent of the court, and the court must hold a detention hearing no later than the end of the next court day after the department files the petition. If the court finds that removal of the youth from the custody of parents is necessary, the court must make a determination regarding the youth’s placement. The department plays a role in this decision, assisting the court in locating and providing the court with placement options, and state law grants youth the right to be placed with a relative or non‑relative extended family member, if an appropriate and willing individual is available.
Until July 2024, in cases where the department could not make an immediate suitable placement for youth, the department had the option to temporarily place youth in its transitional shelter, which CDSS had licensed Alameda County to operate and maintain. The shelter was staffed and managed by WestCoast Children’s Clinic (WCCC), a nonprofit children’s psychology clinic contracted with Alameda County, and the department was responsible to oversee the transitional shelter. The transitional shelter was intended to serve as a child‑friendly environment where youth in the child welfare services system could wait for a more appropriate placement, and it was permitted to hold youth for up to 72 hours before the department could make placement arrangements. The department was required to report to CDSS any instances of youth staying longer than 72 hours. The license terms and agreement for the transitional shelter required the department to provide youth with an individualized assessment of their placement, such as looking for potential relatives for placement options, and for service needs, such as crisis intervention services or psychological screening. The department suspended all operations at the transitional shelter in July of 2024 for several reasons, including its license expiration and a complaint that was made by the city of Hayward in which it was located. As of 2025, the department’s Division Director for Resource Family Approval, Placement, and ILP Support Services stated that the department plans to reopen the shelter at a new location, with a capacity to place 10 youth. The opening date of the new transitional shelter has not yet been determined because the department is waiting for the appropriate building permits.
The Department Has Faced Scrutiny in Recent Years
An Alameda County grand jury report for fiscal year 2022–23 identified shortcomings in the department’s ability to conduct timely investigations. Specifically, it found that in 2022, the department initiated less than half of non‑immediate investigations within the prescribed 10 days following the referral. The grand jury concluded that this recent decrease in investigations that happened within the 10‑day requirement was primarily the result of a 36 percent vacancy rate of child welfare workers in the department’s ER Unit—which handles investigations of child abuse and neglect reports—a shortage driven by the COVID‑19 pandemic. The report acknowledged the efforts the department had made at the time to address the critical staff shortage in the ER Unit but concluded that none had yet provided significant relief. As a result, the grand jury recommended that the department continue its efforts and consider additional extraordinary efforts to recruit and retain child welfare workers.
A 2024 review by CDSS also identified department shortcomings in the areas of identifying timely placements for youth, particularly those with complex needs; lack of documentation of placements, assessments, and services; and high job vacancy rates that create a barrier to family finding. CDSS reviewed case records and conducted a site visit, finding that the department demonstrated an inability to transition youth with the most complex needs to a suitable placement within the required 3‑day time frame. It also found a lack of evidence of children receiving services or support, such as specialty mental health services. CDSS recommended that the department develop policies and procedures that ensure the documentation of placement episodes,4 engagement with preventative services, and engagement with other departments to ensure high quality collaborative case planning. CDSS points to requirements in All County Letters5 and in state law as guidelines for crafting those policies and procedures.
Finally, in June of 2023, the city of Hayward filed a lawsuit against Alameda County and other defendants alleging that the conditions at the transitional shelter constituted a public nuisance and that the county failed to act in the best interest of youth in its care. In particular, the complaint alleged that minors faced the prospect of assault and sexual exploitation, including alleged human trafficking, at the hands of other youth at the shelter, and that daily calls for service to investigate youth who left the shelter without permission or who were engaged in criminal conduct burdened limited local police resources. Hayward filed a notice of settlement in September 2024, and the case was subsequently dismissed.
Audit Results
- High Job Vacancy Rates and Caseloads Have Contributed to Delays in Investigations of Alleged Child Abuse and Neglect
- The Department Has Not Ensured That Interagency Partners Provide Timely Services, Risking the Health and Safety of Foster Youth
- The Department’s Efforts to Connect Youth With Family and Keep Them Safe in Temporary Shelter Have Been Inadequate
High Job Vacancy Rates and Caseloads Have Contributed to Delays in Investigations of Alleged Child Abuse and Neglect
Key Points
- From July 2019 through March 2025, the Alameda County Department of Children and Family Services (department) did not consistently initiate or complete investigations within the required time frames, leaving children in potentially unsafe situations. Although circumstances beyond the department’s control contributed to its late initiation of the investigations we selected for review, its case files did not always contain adequate information describing why investigations were completed late, once started.
- Since July 2019, vacancy rates for child welfare workers have doubled and have more than doubled for child welfare supervisors. Although the department has taken some steps to address its vacancies, it could undertake additional efforts, such as recruiting more entry level staff and addressing some of the concerns of current staff to increase retention.
The Department Has Not Timely Initiated or Completed Investigations of All Referrals for Child Abuse and Neglect Allegations It Received
State law requires the department to operate a 24‑hour emergency hotline to receive and respond to reports of alleged child abuse and neglect. When the department receives such reports, it uses a tool prescribed by the California Department of Social Services (CDSS) to evaluate whether the nature of the allegation requires an in‑person investigation or whether the department can close the referral without further action. The department may close a referral without further action for several reasons, including when a report involves duplicate referrals that contain no new information or when the youth resides in another county. For all other referrals, the department must conduct in‑person investigations, as the text box shows. If the referral indicates that youth are in imminent danger of physical pain, injury, disability, severe emotional harm, or death, the department must conduct an in‑person investigation within 24 hours of receiving the referral (immediate referral). When an allegation could constitute abuse or neglect, but the child is not at imminent risk, state law requires an in‑person investigation within 10 days (non‑immediate referral).
The Department Must Perform Investigations Within Prescribed Time Frames:
Immediate Risk of Abuse, Neglect, or Exploitation: Requires an in‑person investigation within 24 hours. The department must complete the investigation within 30 days of the date of first in‑person contact.
Non‑immediate Risk: Requires an in‑person investigation within 10 days when a child is not in imminent danger, but there is a risk for their safety if the situation is not stabilized at home. The department must complete the investigation within 30 days of the date of first in‑person contact.
Source: Review of state law and CDSS policies.
Delayed Initiation of Investigations
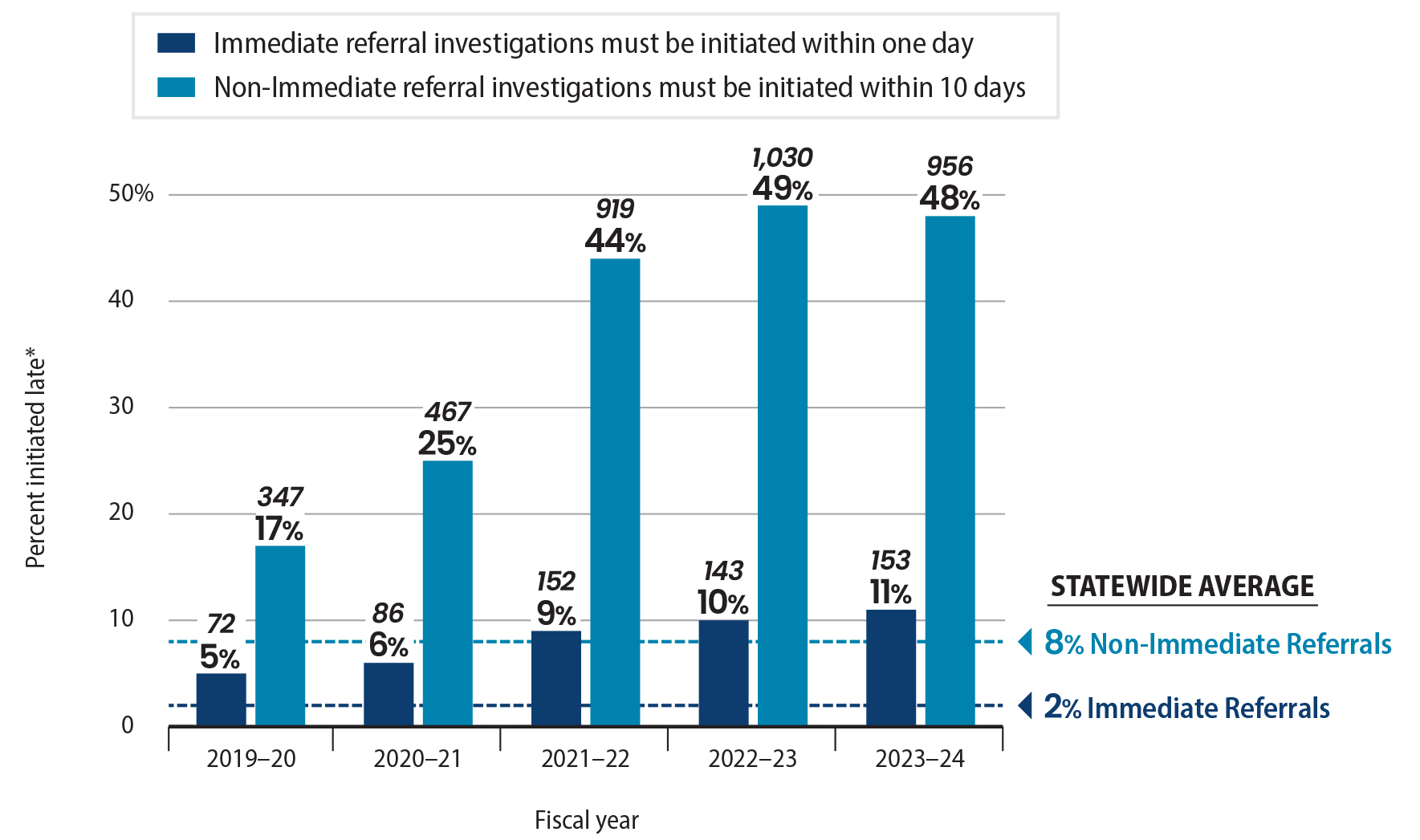
According to the department’s investigations data, the number of immediate and non‑immediate referrals for which it did not initiate investigations within the required time frames more than doubled from fiscal year 2019–20 through fiscal year 2023–24—the most recent fiscal year for which the department could provide complete data.6 Specifically, as Figure 2 shows, the percentage of investigations of immediate referrals that the department initiated after the prescribed 24‑hour time frame increased from 5 percent in fiscal year 2019–20 to 11 percent in fiscal year 2023–24. Similarly, the percentage of non‑immediate referrals for which the department initiated investigations after the prescribed 10‑day period increased from 17 percent in fiscal year 2019–20 to 48 percent in fiscal year 2023–24. Further, these percentages fall far short of statewide averages for the initiation of investigations. According to data published by the University of California, Berkeley and CDSS, the statewide averages for late initiation of investigations of immediate and non‑immediate referrals during this same period were just 2 percent and 8 percent, respectively. We present in Appendix A more detailed information on all referrals, including those that the department had not yet initiated, that the department received for the period we reviewed.
Figure 2
The Department Did Not Initiate Investigations for a Significant Percent of Referrals Within the Prescribed Time Frames
Source: Analysis of Alameda County’s CWS/CMS data.
Note: Although state law requires county welfare departments to respond to any report of imminent danger to a child immediately—or within 24 hours—the CWS/CMS data does not always include time data along with the recorded dates, therefore, our analysis determines immediate referrals to be on time if they were initiated within one day of receiving the referral.
* In addition to the investigations it initiated late, Alameda County had not initiated investigations for between 3 to 6 percent of immediate referrals, and 5 to 16 percent of non‑immediate referrals, it received during the years we reviewed. Appendix A provides a detailed breakdown by year.
Figure 2 is a bar chart that shows that the department did not initiate investigations for a significant percent of referrals within prescribed time frames. The figure shows that in fiscal year 2019-20 the department initiated investigations for 5 percent, or 72 immediate referrals after the required 24-hour time frame. The percentage of late initiation of investigations of immediate referrals increased to 11 percent, or 153 immediate referrals, in fiscal year 2023-24. Similarly, in fiscal year 2019-20, the department did not initiate investigations of non-immediate referrals within the required 10 days for 17 percent, or 347 referrals, which rose to 48 percent, or 956 referrals, in fiscal year 2023-24. The statewide average for not initiating investigations within the required time frames are 2 percent for immediate referrals and 8 percent for non-immediate referrals. A footnote to the figure states that in addition to the investigations it initiated late, Alameda County had not initiated investigations for between 3 to 6 percent of immediate referrals, and 5 to 16 percent of non‑immediate referrals, it received during the years we reviewed. Appendix A provides a detailed breakdown by year. The figure notes that although state law requires county welfare departments to respond to any report of imminent danger to a child immediately—or within 24 hours—the CWS/CMS data does not always include time data along with the recorded dates, therefore, our analysis determines immediate referrals to be on time if they were initiated within one day of receiving the referral. The source of the Figure is analysis of Alameda County’s CWS/CMS data.
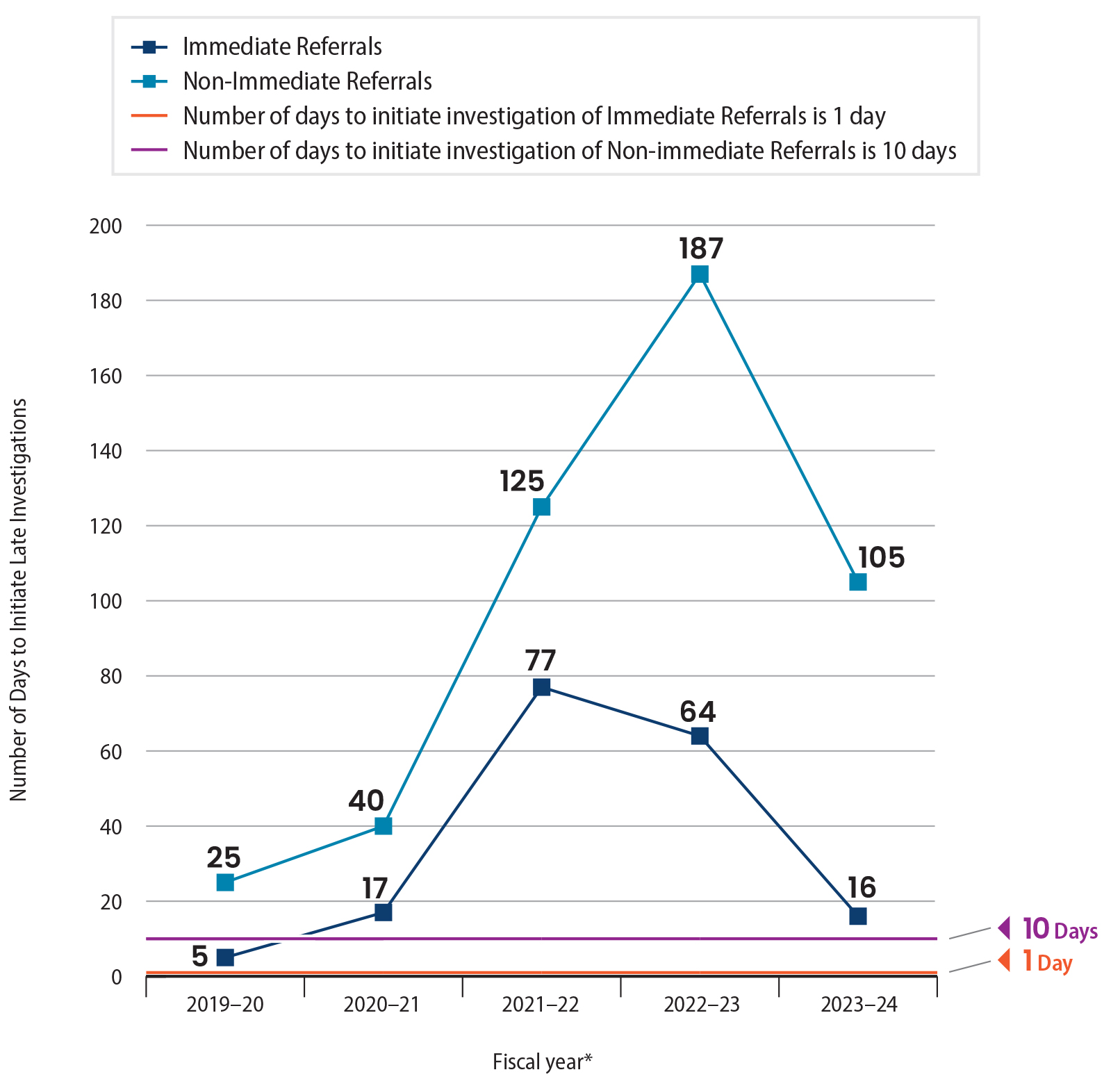
Moreover, for those investigations the department initiated after the prescribed time frames, it has generally taken longer on average to begin these investigations compared to fiscal year 2019–20, as Figure 3 shows. In fiscal year 2019–20, the average number of days to initiate late investigations was five days for immediate referrals and 25 days for non‑immediate referrals. The average number of days of late initiations of investigations for immediate referrals peaked at 77 days in fiscal year 2021–22 and 187 days for non‑immediate referrals in fiscal year 2022–23. Although these averages improved in fiscal year 2023–24 for those cases it closed by April 2024, the department still took an average of 16 days to initiate late investigations for immediate referrals and 105 days for non‑immediate referrals. The department’s inability to initiate investigations within the required time frames threatens the health and safety of the youth residing in Alameda County.
Figure 3
Although Average Days of Late Initiation of Investigations Improved in Recent Years, They Are Still Substantially Higher Than the Required Time Frames
Source: Alameda County’s CWS/CMS Data.
Note: In addition to the investigations it initiated late, Alameda County had not initiated investigations for between 3 to 6 percent of immediate referrals, and 5 to 16 percent of non‑immediate referrals it received during the years we reviewed. Appendix A provides a detailed breakdown by year.
* The State of Emergency proclaimed for the State of California due to the COVID‑19 pandemic was in effect from March 4, 2020, through February 28, 2023.
Figure 3 is a line chart that shows the number of days the department was late in initiating investigations. Immediate referrals must be initiated within one day, and non-immediate referrals must be initiated within 10 days. On average, in fiscal year 2019-20 the department initiated immediate referrals five days late, and non-immediate referrals 25 days late. The average number of days to initiate late investigations increased in fiscal year 2020-21, then again increased significantly in fiscal year 2021-22. In fiscal year 2022-23, the department’s late initiations were at their highest for the audit period—64 days late for immediate referrals and 187 days late for non-immediate. In fiscal year 2023-24, the department initiated immediate referrals 16 days late on average, and initiated non-immediate referrals 105 days late on average. This is much lower than the previous fiscal year but is still much higher than the required time frame. The State of Emergency proclaimed for the state of California due to the COVID-19 pandemic was in effect from March 4, 2020 through February 28, 2023. The Figure notes that in addition to the investigations it initiated late, Alameda County had not initiated investigations for between 3 to 6 percent of immediate referrals, and 5 to 16 percent of non-immediate referrals it received during the years we reviewed. Appendix A provides a detailed breakdown by year. The source of the Figure is analysis of Alameda County’s CWS/CMS data.
Late Completion of Investigations
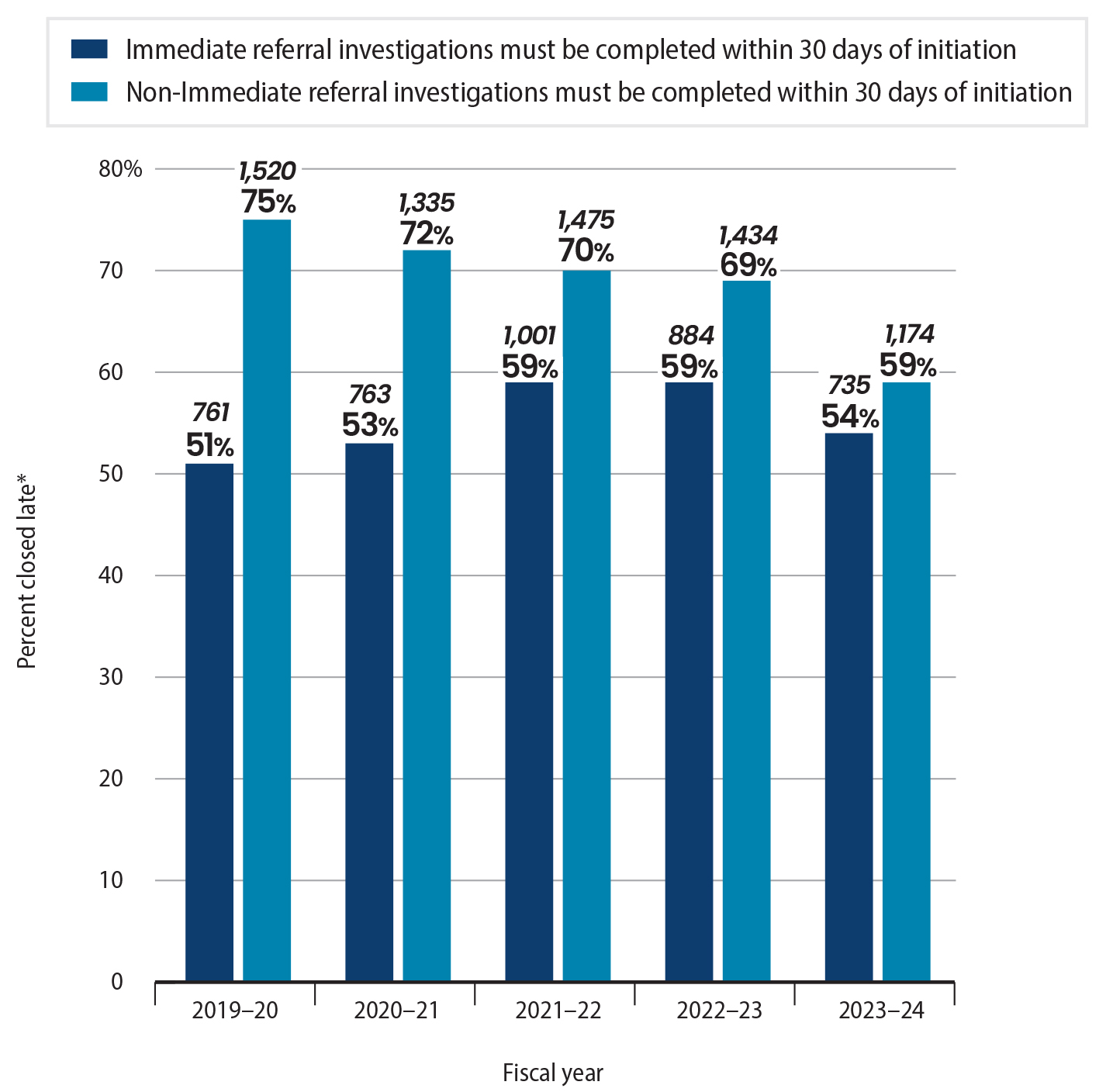
We also found that after initiating investigations, the department did not always complete them within the required time frames. CDSS requires counties to close an investigation within 30 days of the date that the child welfare worker performs an in‑person investigation with the youth. However, the department did not close investigations within 30 days for more than half of all immediate referrals from fiscal years 2019–20 through 2023–24, as Figure 4 shows. Although the percentage of investigations the department closed late for non‑immediate referrals decreased since fiscal year 2019–20, it still completed 59 percent of its investigations of non‑immediate referrals late in fiscal year 2023–24. Further, as Figure 5 shows, the average number of days to complete late investigations has increased compared to the average for fiscal year 2019–20. Unfortunately, there is no data available regarding the statewide averages for completing investigations. Appendix A provides more details regarding the department’s initiation and completion of investigations within prescribed time frames.
Figure 4
The Department Did Not Close Investigations for a Significant Percent of Referrals Within the Prescribed Time Frames
Source: Analysis of Alameda County’s CWS/CMS data.
* In addition to the investigations it closed late, Alameda County still had open investigations for up to 7 percent of the immediate and non‑immediate referrals it received during this period. Appendix A provides a detailed breakdown by year.
Figure 4 is a bar chart showing that the department did not close investigations for a significant percent of referrals within the prescribed time frame. The department must close investigations of alleged neglect and abuse within 30 days of initiation. From fiscal years 2019-20 through 2023-24, the department closed about half of its immediate investigations late—51 percent in fiscal year 2019-20, 53 percent in fiscal year 2021, 59 percent in fiscal years 2021-22 and 2022-23, and 54 percent in fiscal year 2023-24. The department closed 75 percent of its non-immediate investigations late in fiscal year 2019-20, declining each year. The department closed 59 percent of its non-immediate investigations late in fiscal year 2023-24. In addition to the investigations it closed late, Alameda County still had open investigations for up to 7 percent of the immediate and non-immediate referrals it received during this period. Appendix A provides more detailed breakdowns by year. The source of the Figure is analysis of Alameda County’s CWS/CMS data.
Figure 5
Although the Average Days for the Completion of Late Investigations Improved in Recent Years, They Are Still Substantially Higher Than the Required Time Frame
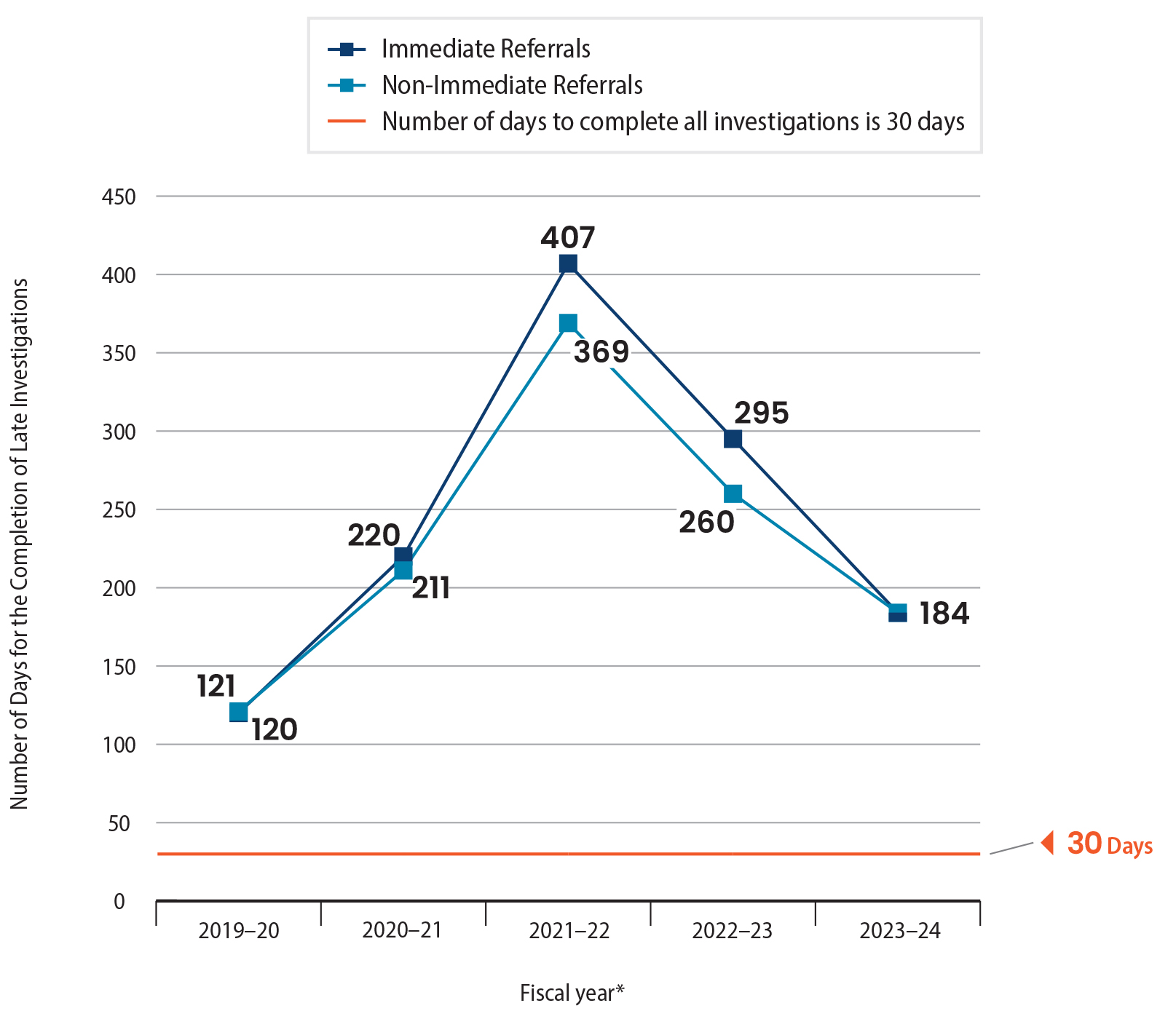
Source: Alameda County’s CWS/CMS Data.
Note: In addition to the investigations it closed late, Alameda County still had open investigations for up to 7 percent of the immediate and non‑immediate referrals it received. Appendix A provides a more detailed breakdown by year.
* The State of Emergency proclaimed for the State of California due to the COVID‑19 pandemic was in effect from March 4, 2020, through February 28, 2023.
Figure 5 is a line chart showing the average number of days the department completed investigations late per fiscal year. The department must complete all investigations within 30 days. It shows that in fiscal year 2019-20, the department completed investigations 120 days late for immediate referrals and 121 days late for non-immediate referrals. The average number of days rose sharply in fiscal year 2021-22, to 407 days late for immediate referrals and 369 days late for non-immediate referrals. In fiscal year 2023-24, the number of days late reduced to 184 for both immediate and non-immediate referrals. It also shows that the State of Emergency proclaimed for the State of California due to the COVID-19 pandemic was in effect from March 4, 2020, through February 28, 2023. The Figure notes that in addition to the investigations it closed late, Alameda County still had open investigations for up to 7 percent of the immediate and non-immediate referrals it received. Appendix A provides more detailed breakdowns by year. The source of the Figure is analysis of Alameda County’s CWS/CMS data.
Reasons for Delays in Cases We Reviewed
To assess the reasons for the delays in the department’s initiation and completion of investigations, we reviewed a selection of investigations of 10 immediate referrals and 10 non‑immediate referrals—for a total of 20 referrals. We reviewed case file documents, case worker notes, and interviewed staff to determine the cause of the delays and whether the department’s efforts were appropriate. We found that the department did not initiate an investigation for one of the 10 immediate referrals within 24 hours of receiving it, and did not initiate an in‑person investigation of four of the 10 non‑immediate referrals within the required 10 days, as the text box shows. Specifically, the department made an in‑person contact with the youth involved in the one immediate referral three days after receiving the allegation. For three of the four non‑immediate referrals, the department did not make in‑person contact with the involved youth until as many as 28 days after receiving the referral, and in the fourth instance, the department could not reach the family or the youth at all.
Timeliness of First In‑Person Contact for 20 Referrals We Reviewed
Late First In‑Person Contact: The department made first in‑person contact for one of 10 immediate referrals and four of 10 non‑immediate referrals after the required time frames.
Source: Review of investigation files.
In all five instances, the delays in initiating required investigations were because of circumstances beyond the department’s control. For example, according to notes in the case file for the one immediate referral for which the department did not initiate an in‑person investigation within 24 hours, the department staff attempted to meet with the youth at school on the same day that the department received the report of alleged abuse and neglect; however, the youth was not at school. The staff also called the parent of that youth on the same day and learned that the parent was also not available because of a personal appointment. Ultimately, the child welfare worker scheduled and met with the youth and the parent three days after receiving the referral.
The department faced similar circumstances for three of the four non‑immediate referrals for which it did not initiate an in‑person investigation within the required 10 days. For one of these referrals, the child welfare worker made a few attempts to contact the parent of the youth within 10 days, including leaving voice messages and visiting the home. The department staff was able to contact the parent on the telephone and schedule an in‑person meeting just before the 10‑day period expired. However, the parent was then unable to meet as scheduled because of health reasons, and the child welfare worker had to reschedule and meet with the parent 20 days after the department received the non‑immediate referral. Similarly, the child welfare worker attempted, but was unable, to contact the youth for two other non‑immediate referrals within 10 days of receiving the referrals, resulting in no in‑person contact for almost a month after receiving the referrals. We recognize the challenges the child welfare workers face in contacting the youth and families; however, delays in investigating allegations of child abuse and neglect risk the health and safety of the youth.
For the remaining one non‑immediate referral that the department did not close within the required time frame, despite repeated attempts, it could not contact the family or the youth at all. The referral notes show that the child welfare worker made four separate attempts to contact the youth and the family, including telephone calls, text messages, and a letter to the mother’s last known address. Ultimately, the child welfare worker noted that she was unable to locate the family and closed the referral. This was an appropriate action—according to CDSS policy, the child welfare worker may close the referral if attempts to locate the family are unsuccessful.
Further, as the text box shows, in 10 of the 20 investigations we reviewed, the department exceeded the time frame for closing investigations, which is 30 days from the first in‑person contact. For those 10 investigations, the department took from 42 to 476 days—with an average of 275 days—to conclude the investigations.
Timeliness of Completing 20 Investigations We Reviewed
Late Investigation Completion: The department closed investigations for four of 10 immediate referrals and six of 10 non‑immediate referrals after the 30‑day requirement.
Source: Review of investigation files.
Notes in the case files for seven of the 10 late investigations did not provide any details to determine the reasons for the late closure of investigations. For example, according to the case file notes, the department received a non‑immediate referral in December 2023, and the child welfare worker assigned to the case made the first in‑person contact within 10 days, as required. However, the child welfare worker did not complete the safety and risk assessment until November 2024. As such, the investigation did not close until nearly a year after the first in‑person contact. Nothing in the case file provided any information for the late assessment. The director of the Prevention and Intake Services Division stated that the child welfare worker did not complete the assessment in a timely manner, but could not provide any further explanation.
In the remaining three cases, the child welfare worker completed the investigation within 30 days and recommended closing the three referrals with no further agency involvement. However, the assigned supervisor did not review and approve the recommendations until after the 30‑day period had passed. The assistant agency director for Alameda County Social Services Agency (assistant agency director), who manages the department, confirmed that the department needs to close its investigations in a timely manner consistent with state law and CDSS requirements, which require supervisory signoff. She noted that staffing issues in the department created a situation in which the department could not keep up with referrals. As we describe in the next section, the department has been experiencing high staff and supervisor vacancy rates, including a 35 percent child welfare worker vacancy rate in fiscal year 2023–24. Department management cited these high vacancies and large caseloads as the reason for the delays in responding to and investigating referrals in a timely manner.
We also reviewed whether the department appropriately closed reports of alleged child neglect or abuse that it determined did not require further investigation. The department uses a tool prescribed by CDSS when determining whether to refer a report of neglect or abuse for further investigation. We selected 10 reports of alleged child neglect or abuse that the department closed without any in‑person investigation. The department appropriately closed five reports for which the CDSS‑prescribed tool recommended closing without an in‑person investigation. However, the department overrode the tool’s recommendation to conduct in‑person investigations for the remaining five reports of alleged neglect or abuse.
For four of the five reports for which the department chose to deviate from the tool’s recommendation, we found that it documented a reasonable explanation for doing so. For example, in one instance, although the tool’s recommendation was to refer the report for an in‑person investigation, it had received a duplicate allegation regarding the family one day earlier. As such, the department overrode the recommendation for the report we selected and closed it by combining the two reports of neglect or abuse. The department recommended an in‑person investigation of the allegations for the combined report.
Although the department had a valid reason for closing the remaining one report for which the department overrode the CDSS‑prescribed tool’s recommendation to perform an in‑person investigation, it unnecessarily delayed its investigation of the underlying allegations. Despite the CDSS‑prescribed tool’s recommended action to conduct an in‑person investigation, the department closed a report it received in April 2023 alleging parents’ negligence to follow up on a youth’s important medical appointments. The division director of the Prevention and Intake Services Division (division director) stated that at the time it received the report in April 2023, the child welfare worker assigned to the report went on leave, and as a result the department did not timely complete the intake of that report. The department noted in the investigation case file that it received a similar report involving the same family a month later, in May 2023. Case file notes stated that the department chose to combine the two reports and close the April report. The department recommended an in‑person investigation for the May 2023 report. By delaying the review of the April report until it received another report in May, the department potentially jeopardized the youth’s health and safety.
The Department Has Not Taken Sufficient Action to Address Its Increasing Staff Vacancy Rates and High Caseloads
To review foster child placements and investigate child abuse claims, state law requires that child welfare agencies maintain and operate a 24‑hour response system. The department hires child welfare workers and supervisors to provide intake services for child abuse and neglect allegations, to investigate child abuse and neglect referrals, and to provide placement and foster care services for youth who are determined to be dependents of the court.
The department has experienced high vacancy rates for its child welfare workers and supervisors. The department’s vacancy rate for child welfare workers doubled from 17 percent in fiscal year 2019–20 to 34 percent in fiscal year 2024–25, as Figure 6 shows. Similarly, its vacancy rate for supervisors more than doubled from 8 percent in fiscal year 2019–20 to 18 percent in fiscal year 2024–25.
Figure 6
The Vacancy Rate of Child Welfare Workers and Child Welfare Supervisors Has Significantly Increased From Fiscal Years 2019–20 Through 2024–25
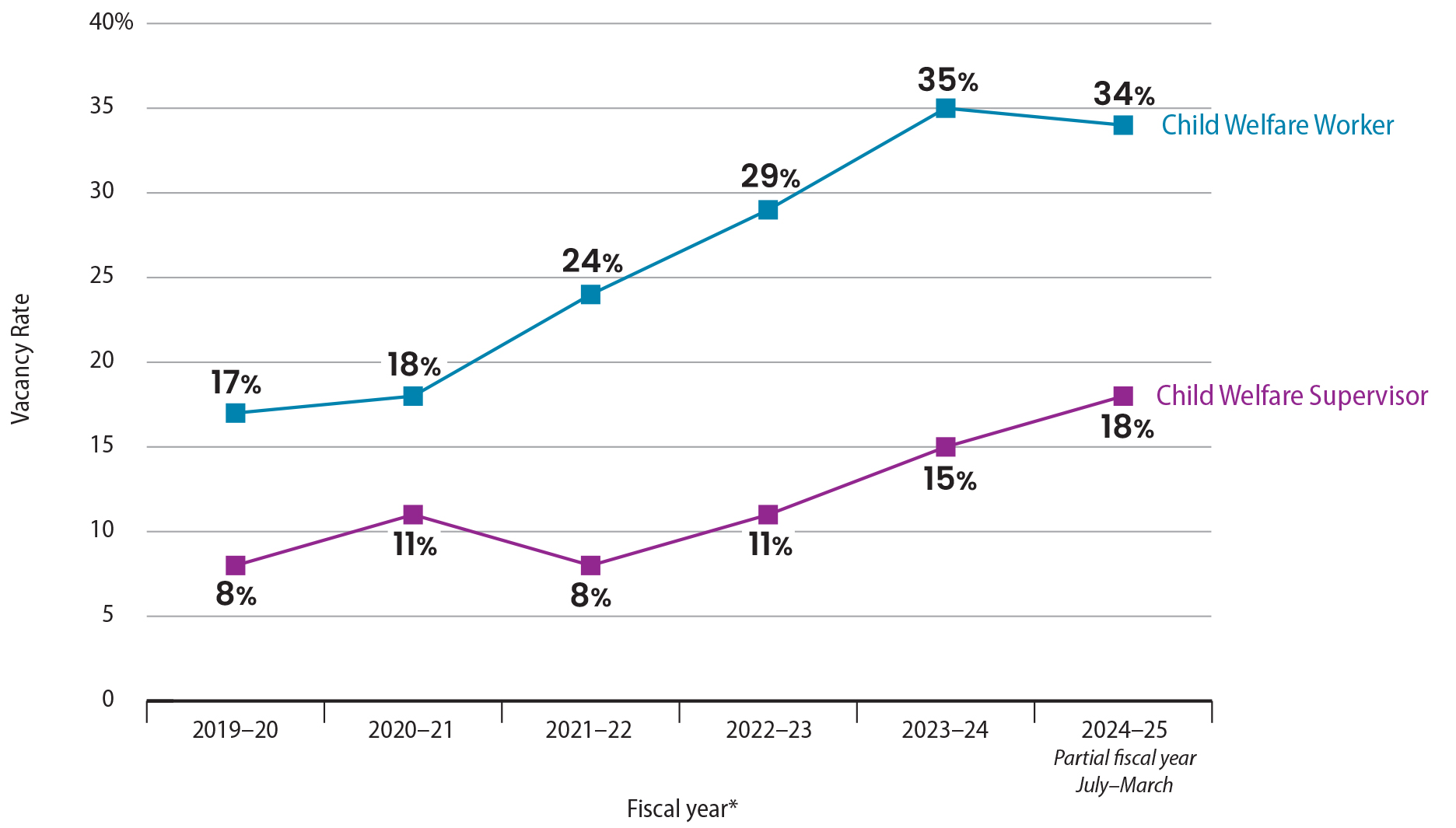
Source: Review of department position control documents.
Note: During all fiscal years shown, the department had 290 authorized positions for child welfare workers, and 77 for child welfare supervisors.
* The State of Emergency proclaimed for the State of California due to the COVID‑19 pandemic was in effect from March 4, 2020, through February 28, 2023.
Figure 6 is a line chart showing the vacancy rate of child welfare workers and child welfare supervisors has significantly increased from fiscal years 2019–20 through 2024–25. In fiscal year 2019-20, the department had a vacancy rate of 17 percent for child welfare workers and 8 percent for child welfare supervisors. The vacancy rate for child welfare workers increased each year through fiscal year 2023-24, where it reached 35 percent. Partial year data for fiscal year 2024-25 shows a decrease of vacancy rates for child welfare workers to 34 percent. The footnote stated that fiscal year 2024-25 is based on data for July 2024 through March 2025. Child welfare supervisor vacancies rose to 11 percent in fiscal year 2020-21, fell to 8 percent in fiscal year 2021-22, then rose steadily to 15 percent in fiscal year 2023-24 and to 18 percent as of March 2025. A footnote states that the State of Emergency proclaimed for the State of California due to the COVID-19 pandemic was in effect from March 4, 2020, through February 28, 2023. The Figure notes that during all fiscal years shown, the department had 290 authorized positions for Child Welfare Workers, and 77 for Child Welfare Supervisors. The source of the Figure is a review of department position control documents.
In fact, Alameda County has experienced a higher vacancy rate for child welfare workers compared to other nearby counties. To determine whether Alameda County’s vacancy rates were comparable to a selection of three counties also located in the Bay Area—Contra Costa, San Francisco, and Santa Clara—we asked CDSS to provide us with vacancy rates for child welfare worker positions for the other three counties from fiscal years 2019–20 through 2023–24. We learned that Alameda County experienced an average vacancy rate in child welfare supervisors of 11 percent during the five‑year audit period, which was lower than Contra Costa’s 18 percent average vacancy rate and San Francisco’s 15 percent rate. However, as Figure 7 shows, Alameda County’s vacancy rate for child welfare workers was higher than the other three counties during the period we reviewed. The three counties reported that they had an average vacancy rate for child welfare workers below 20 percent during the five years we reviewed. However, Alameda County experienced an average of 25 percent for child welfare workers during this same period. San Francisco County, which had the second highest vacancy rates in recent years, reported its vacancy rates for child welfare workers at 29 percent for fiscal year 2023–24, which is still less than Alameda County’s 35 percent vacancy rate for its child welfare workers during the same year.
Figure 7
The Child Welfare Worker Vacancy Rates in Alameda County Have Been Consistently Higher Compared to Other Bay Area Counties
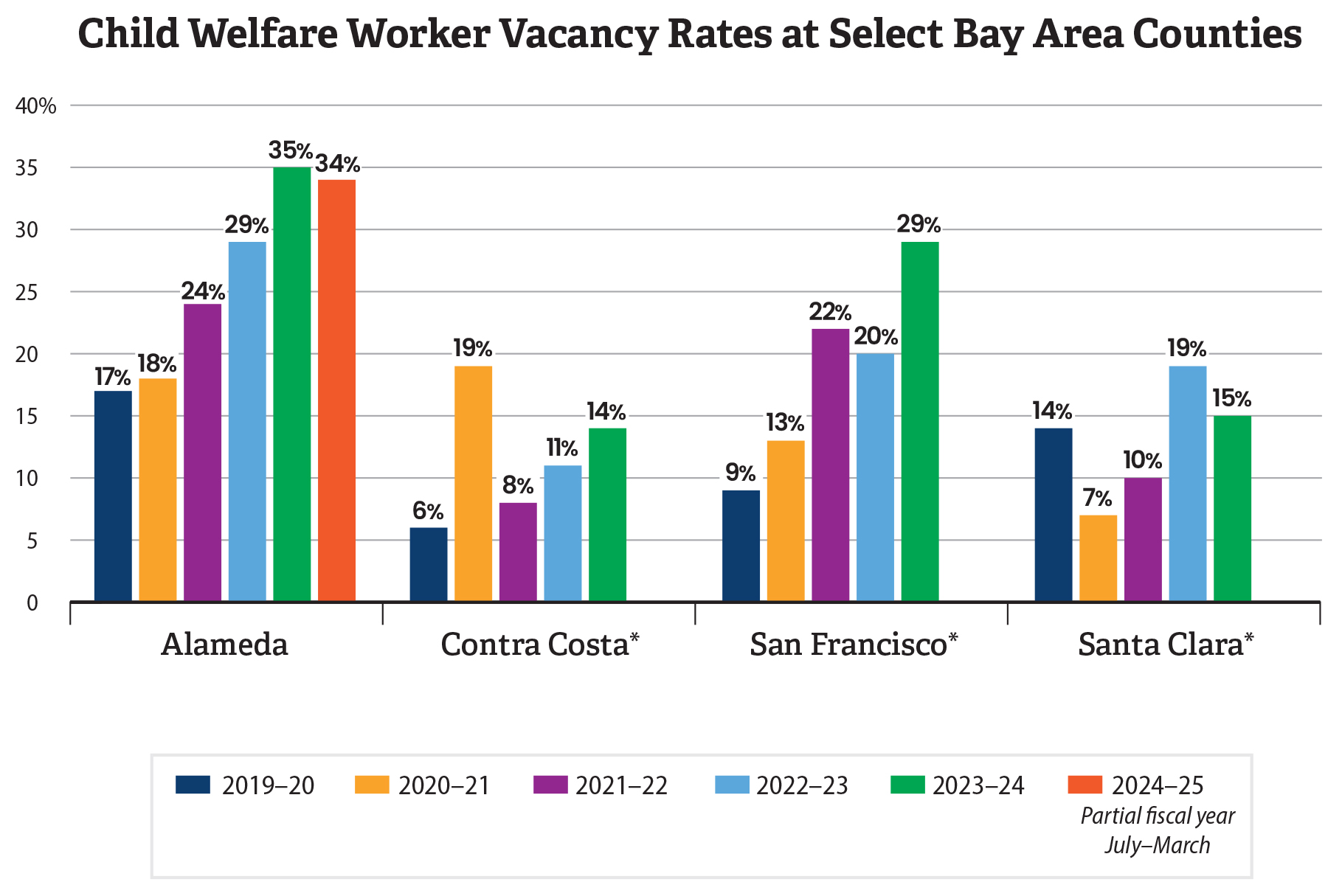
Source: Review of the department’s position control data and CDSS’s annual training surveys.
Note: For Alameda County, we used the department’s position control data. For all other counties, we obtained data from CDSS’s annual training surveys.
* CDSS did not yet have fiscal year 2024–25 data for Contra Costa, San Francisco, and Santa Clara counties.
Figure 7 is a bar chart showing that the child welfare worker vacancy rates in Alameda County have been consistently higher compared to other Bay Area counties. The Figure shows child welfare worker vacancy rates from fiscal years 2019-20 through 2023-24 and partial year (July to March) for fiscal year 2024-25 for Alameda, Contra Costa, San Francisco, and Santa Clara counties. For each fiscal year, Alameda County’s vacancy rate is substantially higher than the nearby counties. In fiscal year 2019-20, vacancy rate for Alameda County was at 17 percent, Santa Clara at 14 percent, San Francisco at 9 percent, and Contra Costa County at 6 percent. Alameda County reached its highest vacancy rate in fiscal year 2023-24 at 35 percent; while the vacancy rate in the same fiscal year for Santa Clara County was 15 percent, San Francisco County was 29 percent, and Contra Costa was 14 percent. From June 2024 through March 2025, Alameda County had a 34 percent child welfare worker vacancy rate. A footnote states that CDSS did not yet have fiscal year 2024–25 data for Contra Costa, San Francisco, and Santa Clara counties. The Figure notes that for Alameda County, we used the department’s position control data. For all other counties we obtained data from CDSS’ annual training surveys. The source of the Figure is review of the department’s position control data and CDSS’s annual training surveys.
The assistant agency director attributed the department’s high vacancies to a nationwide shortage of child welfare workers and the nature of the work. She noted that the demand for social workers, particularly for child welfare workers, is growing faster than the supply of individuals willing to do the work. In fact, a study based on data from the National Child Abuse and Neglect Data System confirms that public child welfare agencies face challenges, including high workforce turnover.7 Specifically, the study found that from 2003 through 2015, the median turnover rate for all states was from 14 percent to 22 percent and that case workers stayed on the job for a median of 1.8 years. The assistant agency director explained that the COVID‑19 pandemic resulted in challenges in recruitment and retention because of factors such as anxiety about conducting home visits and increased stress. She also noted that the intense and often traumatic nature of the work, with exposure to challenging situations involving youth and families, can lead to stress and burnout among child welfare workers.
The department’s child welfare workers we interviewed also identified stress as one of the biggest challenges leading to staff turnover. We spoke with four child welfare workers at the department to understand their perspectives on high vacancy rates. Staff identified department culture and lack of resources as some of the challenges, as the text box shows. Staff told us that because they often assist families experiencing extreme poverty, any inability to provide necessary resources or services to families due to unclear rationale for limits on what the department can provide to families puts undue stress on child welfare workers because they are the family’s primary contact with the department. They also told us that certain department policies place undue stress on them. For example, staff stated that department policy requires that they conduct in‑home, unannounced interviews for every family member, even if they were not directly involved in the cause for investigation, which often requires significant travel that can take up much of a workday. The staff offered some suggested changes to assist in lowering the high vacancy rates, including creating a new pay differential for daytime Emergency Response (ER) Unit workers because of the added safety concerns and intensity of the work, and not requiring in‑home, unannounced interviews for family members not directly involved in the incident being investigated.
Some of the Challenges Leading to Staff Turnover That Child Welfare Workers We Interviewed Identified Involved Problems With Department Culture and Resources:
- Upper management does not effectively communicate the reasons for certain policies, procedures, or priorities, leaving workers frustrated and in the dark.
- Upper management does not take child welfare workers’ concerns and ideas for improving the department seriously, nor do they offer many concrete avenues for workers to express those concerns or ideas, other than to their direct supervisor.
- Upper management does not understand the reality of the day‑to‑day work the job requires, especially when workers are going above and beyond to complete their work on time.
- Delays in payment processing for foster parents put undue stress on child welfare workers because they are a foster parent’s primary contact with the department.
Source: Interviews with selected child welfare workers.
In 2023, the department identified similar feedback through exit interviews with employees who resigned, as well as through a workforce survey. Specifically, the department found that emotional exhaustion, demands and expectations of the job, work culture, and insufficient resources to complete work, were some of the key reasons that employees would consider ending their employment or changing their positions. Nearly 60 percent of the respondents agreed that there is not clear and timely communication between management and frontline staff about department policy changes. Further, nearly 70 percent of the respondents agreed that work is not adequately distributed.
Moreover, in fiscal year 2022–23, a report by the Alameda County grand jury identified several factors that contributed to the department’s high vacancy rates, including a lack of supervisor support and mentoring. In particular, the report noted that some supervisors do not devote enough time and effort to support and mentor new staff in learning to manage caseloads and perform investigations. The report recommended that the department take steps to increase work‑related support for child welfare workers by requiring supervisors to schedule regular check‑ins and provide timely guidance and mentoring for caseload management, among other things. According to the assistant agency director, although the department has implemented the grand jury’s recommendations, the recommendations did not address the issue of not having a sufficient applicant pool for child welfare worker positions.
The assistant agency director does not believe that lack of funding or salaries have contributed to the department’s vacancies. She believes that the county’s salaries for its child welfare workers are competitive compared to similar positions in other Bay Area counties. Although she acknowledged that some staff are leaving for positions in other counties, she does not believe that pay is the only reason staff are leaving. She stated that staff are also leaving for positions in other Alameda County agencies where the pay is less, but the workload is more balanced. Our review of child welfare worker salaries in Contra Costa, Santa Clara, and San Francisco found that the department’s salaries were generally comparable with the other Bay Area counties, considering the cost of living. In fact, the employee feedback that the department compiled in 2023 found that employees cited pay and benefits as the key reason for maintaining their employment.
The high number of vacancies in Alameda County has resulted in higher caseloads for child welfare workers and has hindered the department’s ability to meet the needs of the county’s youth and families. The assistant agency director noted that the department’s high vacancy rates are increasing staff caseloads and causing an emotional burden on staff and managers who are responsible for assisting youth and families. In fact, a fiscal year 2022–23, Alameda County’s Grand Jury Final Report found that the department’s high vacancies led to additional stress and higher caseloads of emergency response child welfare workers at the department, which in turn resulted in delays in investigating the non‑immediate referrals for child abuse and neglect investigations.
In recent years, child welfare workers’ caseloads have exceeded agreed‑upon guidelines for the Emergency Response Program administered by its ER Unit, which is responsible for investigating reports of child neglect and abuse. As the text box shows, the union agreement with the county in 2015 set certain caseload guidelines for child welfare workers, depending on their classification.8 We obtained case assignment data from the department to assess its adherence to the caseload guidelines. Specifically, to assess caseloads for the Emergency Response Program, we identified the number of new emergency response cases the department assigned to each staff during each calendar month of our audit period. We aggregated the number of instances, or staff‑months, for which individual staff had new emergency response caseloads exceeding 15 cases. For example, if two staff each had a total new emergency response caseload of more than 15 during a month, we counted that as two staff-months with caseload exceeding the guidelines of 15 cases. As Table 1 shows, from fiscal years 2019–20 through 2023–24, the department consistently assigned new monthly emergency response caseloads to staff that exceeded the caseload guidelines, with 15 to 30 percent of all staff‑months exceeding the guidelines each year. In contrast, as Appendix B shows, we found that the department generally met the caseload guidelines when assigning cases for the family maintenance and family reunification programs.
The Union Agreement With Alameda County Set Certain Caseload Guidelines for Child Welfare Workers
Emergency Response Program: No more than 15 new cases per month.
Family Maintenance Program: No more than 28 cases per day.
Family Reunification Program: No more than 19 cases per day.
Source: Alameda County’s agreements with the union executed in 2015.
The department has attempted some strategies to address its vacancies and related high caseloads. For example, in November 2022, it used involuntary staff transfers to help address open referrals and reduce caseloads in the ER Unit. According to the division director, the plan was to rotate seven staff from other units to the ER Unit for one year after which they could return to their previous roles in their former units. However, she noted that most staff either resigned or went out on leave before the end of the year. Ultimately, she believed that the strategy did not provide much progress in addressing referrals, and it severely harmed staff morale. In addition, the department explained that in 2023, it implemented another rotational program to help address the backlog of referrals created when staff left the department. This rotation program included transferring six staff on a three‑month rotation to the ER Unit to focus on existing open referrals. The division director explained that the program ended in fall 2024 when the department had addressed the backlog of referrals for the workers who had left.
Although the department has expanded its recruitment of the Child Welfare Worker I (CWW I) position in recent years, it is still able to hire more staff at this entry level position, which may be easier to recruit. In 2023, the department expanded its recruitment beyond the Child Welfare Worker II (CWW II) position, which requires a master’s degree, to include the CWW I position, which requires only a bachelor’s degree with two years of experience in specific areas. The first cohort of individuals hired into the CWW I position joined the department in September 2023 with a total of 15 new staff, of which it assigned nine to the dependency investigation and family maintenance programs of the ER Unit. As of July 2025, the department had 32 child welfare workers in the CWW I position, with 26 of them assigned to the ER Unit—this number comprises about 29 percent of all child welfare workers in the division. The state requirement for an emergency response program is that at least 50 percent of workers should have a master’s degree, and the other 50 percent may have only a bachelor’s degree. To reduce the existing vacancy gap in its ER Unit, we believe that the department can hire more individuals in the CWW I position, which has less educational requirements and may be easier to recruit. The assistant agency director noted that entry level child welfare workers require more direct oversight and involvement by supervisors. For this reason, she noted that it is preferable to hire more experienced individuals into the CWW II position. However, we believe that the department could implement a practice in which new child welfare workers can shadow more experienced staff and reduce the time supervisors need to spend with the new staff. This approach could thereby allow the department to hire more staff at one time. Even though the department says that it has tried voluntary shadowing in the past, we believe that it could formalize the shadowing process and make it mandatory for new staff.
The Department Has Not Ensured That Interagency Partners Provide Timely Services, Risking the Health and Safety of Foster Youth
Key Points
- The department has not ensured that youth in foster care (foster youth) receive needed services in a timely manner because it has not consistently documented and tracked the frequency and the timeliness of services provided by its interagency partners or the department’s contractors. We reviewed 125 selected services that 36 youth needed to receive and found that the department did not document when 65 services were requested or delivered—preventing us from determining whether the youth received those services in a timely manner. Case files lacked documentation to determine the timeliness of services involving 89 percent of regional center services and more than 90 percent of mental health services.
- In cases for which sufficient documentation was available for our review, we found that the department did not always ensure timely provision of services for some youth. Specifically, of the 60 selected services that had sufficient documentation, we found that youth received 27 of them only after delays. For example, the provision of sexual education classes had the longest average delay of 456 days.
Lack of Documentation Prevents the Department From Demonstrating That Foster Youth Received Timely Services
State law requires that counties establish MOUs with certain public and private partners to collaborate on the delivery and management of services to foster youth. State law requires the county to establish the MOU to ensure that youth in foster care receive coordinated, timely, and trauma‑informed services. Alameda County established an MOU in May 2022, which includes the partners for its interagency leadership team (ILT), as Figure 8 shows. The department’s partners on the MOU are the Alameda County Behavioral Health Department, the Alameda County Office of Education, the Regional Center of the East Bay, and the Alameda County Probation Department. These interagency partners provide foster youth with certain services, such as education case management services; services for youth with intellectual and developmental disabilities; and the coordination of referrals, screening, eligibility, and authorization for therapeutic care for youth with complex emotional and behavioral needs. For services that the department regularly requires and that its interagency partners do not provide, such as child abuse prevention and treatment services, the department contracts with third parties, and such contracted services can include independent living services, transitional housing, and youth employment programs.
Figure 8
The Department Established an Interagency MOU That Allows It to Partner With Other Agencies and Contractors to Provide Coordinated Services to Foster Youth
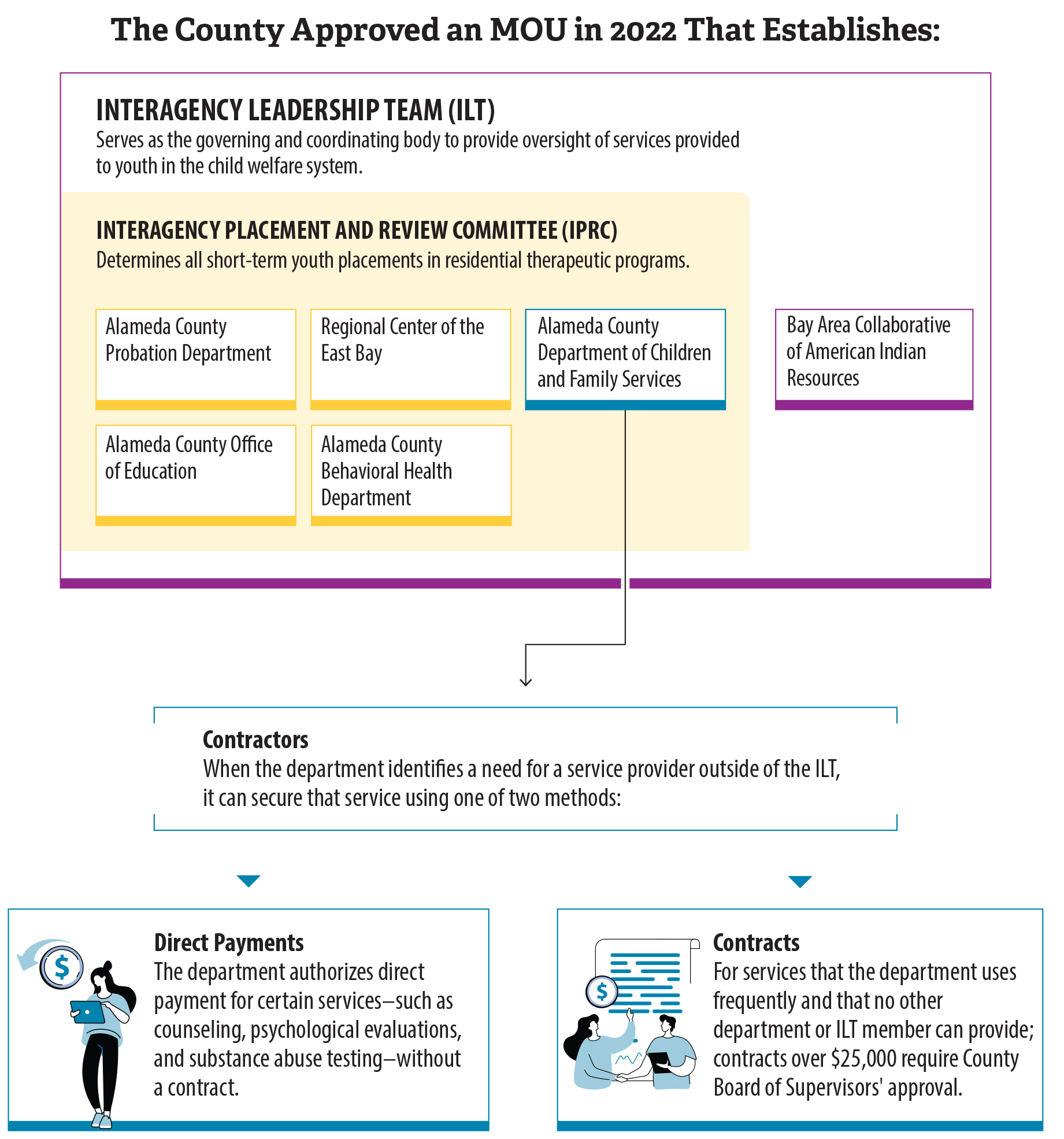
Source: Auditor review of department contracts.
Figure 8 is a color-coded flow chart showing that the department established an interagency MOU that allows it to partner with other agencies and contractors to provide coordinated services to foster youth. A box shows the members of the Interagency Leadership Team (ILT) made up of Alameda County Probation Department, Alameda County Office of Education, Alameda County Behavioral Health Department, Alameda County Department of Children and Family Services, Regional Center of the East Bay, and the Bay Area Collaborative of American Indian Resources. The ILT Serves as the governing and coordinating body to provide oversight of services provided to youth in the child welfare system. All the members of ILT, except the Bay Area Collaboration of American Indian Resources, are included within another box labeled Interagency Placement and Review Committee within the ILT box. An arrow pointing from the Alameda County Department of Children and Family Services to a box titled “Contractors” that is outside the ILT box. This box states that when the department identifies a need for a service provider outside of the ILT, it can secure that service using one of two methods. There are two boxes below the “Contractors” box: one for Direct Payments and one for Contracts. The Direct Payment box states that the department authorizes direct payment for certain services–such as counseling, psychological evaluations, and substance abuse testing–without a contract. The Contract box states that for services that the department uses frequently and that no other department or ILT member can provide; contracts over $25,000 require County Board of Supervisors’ approval. The source of the Figure is auditor’s review of department contracts.
Although timely support services are critical to ensuring youth’s health and safety, the department has not consistently documented and tracked the frequency and the timeliness of services provided through its interagency partners or the department’s contractors. For our review period of fiscal years 2019–20 through 2024–25, we reviewed 125 selected services involving 36 youth. For 65 of the 125 services we reviewed, we did not find necessary documentation that would allow the department to know whether youth received these services within agreed‑upon frequencies and time frames, as Table 2 shows. We expected the department to include in its hard copy case files, or in its electronic case management system, documentation or detailed notes to identify the dates when specific services were requested for the youth and the dates those services were actually provided. However, the department often did not document when services were requested or provided, preventing us from evaluating timeliness. Further, without this information, the department cannot know the reasons why services were delayed and take the steps necessary to make improvements.
Services related to mental and behavioral health lacked the most documentation. Individual case plans and court documents outline the specific service needs of a youth. The department creates a case plan that highlights the family’s case goals and the services the youth and their family members would need to meet the needs of the youth and to meet the case plan goals. For example, the department may determine that a youth needs weekly therapy through the county’s Behavioral Health Department, educational support services through the county’s Department of Education, and other support services through contracted service providers. The department may further determine that the youth should receive health and dental services required by the Child Health and Disability Prevention (CHDP) program.9 The department identifies specific time frames for providing these services in the case plan. During status hearings, which are required to occur no less frequently than every six months, the court considers the department’s compliance with the case plan.
Hard copy case files and electronic case management system records for all 10 mental health service referrals the department made and we reviewed lacked treatment summaries identifying the dates when the services were provided, or email confirmations from the service providers or partner agencies, to determine whether the youth received timely services. Similarly, none of the case files for the nine mental or behavioral health services provided by the county’s Behavioral Health Department, an interagency partner of the department, contained similar documents that would allow the department to determine whether youth received timely services. The department maintained better documentation for transitional housing services, health services, and education services, allowing it to determine whether youth received such services within acceptable time frames.
During monthly check‑ins with the youth, child welfare workers gather information about services and document them in contact notes, which remain as part of the youth’s case file. Although child welfare workers generally made their monthly visits to foster youth, existing contact notes included inconsistent or inadequate details about the frequency and dates of services youth received. For example, documentation in the case file of one youth who was receiving mental health services through a referral by the department attested to the youth receiving weekly therapy sessions, but the case file contained no supporting documentation, such as treatment summaries or communication from providers or agency partners about the treatment provision, to confirm attendance or identify any gaps in services. The department could not explain why such documentation was not in the case files.
Similarly, case file documentation for youth receiving regional center services did not adequately demonstrate regular service provision. For example, we reviewed a case in which a youth was receiving services from a regional center. The regional center created an Individual Program Plan (IPP) for the youth. The IPP is a written document that includes the individual’s goals and future plans, and it also includes all services and support necessary to meet those goals. The regional center develops and periodically updates the IPP with the agreement of the youth, the parents, the legal guardian, or the conservator, as appropriate. The IPP called for the regional center’s case manager to provide support and attend Individualized Education Plan (IEP) meetings at the youth’s school, and an annual meeting with parents to reassess the youth’s need for services. Child welfare workers made monthly contact with the youth. However, the contact notes only discuss the youth’s IEP meeting on one occasion; therefore, it is unclear whether the case manager attended all IEP meetings. Further, the contact notes do not indicate whether an annual service reassessment occurred. We would have expected to see documentation for all IEP meetings and for at least one reassessment meeting per year. The department’s assistant agency director and a management analyst acknowledged that child welfare workers may not always provide details in contact notes. In the absence of specific and consistent documentation, the department cannot know whether youth receive timely services and cannot meaningfully intervene to ensure that youth receive critical services from its interagency partners.
In addition, the department did not always obtain necessary documents, such as the youth’s IPP, to identify those services a youth with developmental disabilities should receive from regional centers. For youth who are in the foster care system or at risk of entering foster care, the department must collaborate with the regional center to ensure that such youth receive timely services needed to achieve state welfare goals. However, of the 18 cases we reviewed for foster youth who were receiving regional center services, the department did not have the IPP in 16 cases. Without the IPP, the department cannot identify the services that the regional center agreed to provide and cannot determine whether the foster youth received those services. This lack of information creates a risk that youth do not receive services that will help them live productive and independent lives.
Although the department’s policies include general guidelines for staff to contact regional centers and refer youth to a regional center service if they identify the need, the department lacks policies and practices for tracking the number of its youth who use regional center services, nor does it have procedures requiring staff to document efforts to contact the regional centers. The department also asserted that it is not always possible to document the actual provision of services because it cannot compel regional centers to provide necessary documents. In addition, the department is often not a party to the IPP, and those rights often remain with the parents. Although child welfare workers ask for copies of all signed documents, they may not receive copies at the time and additional follow‑up may be necessary. Generally, regional centers do not coordinate planning or assessment needs with the department. However, without documenting its attempts to contact partners and request documentation, the department cannot be certain that it has made all necessary efforts to ensure that youth receive necessary services.
However, the department’s MOU with its partner agencies allows the department to take steps to receive needed documentation on services from other MOU partners. Alameda County’s MOU states that partners will attempt in good faith to resolve any dispute or disagreements, with local directors, chiefs, and department heads seeking to settle relevant disputes by focusing on the shared vision, values, and practices of the MOU. The provision further states that if a consensus cannot be reached, decisions may be made by a simple majority vote of the ILT members. We believe that the MOU’s dispute resolution provision allows the department to propose a provision on information sharing, including information on services provided to youth, to ensure timely and coordinated delivery of services. Further, if disagreements exist between MOU members on the details of the proposed provision, the dispute resolution process would allow the MOU partners to reach consensus, or a majority opinion, on how partners may share service information in a timely manner. The assistant agency director stated that the department cannot force the change. She explained that the agency can suggest the change, but the other parties would need to review, and they could reject it. Nevertheless, the department has not attempted to make the change to the MOU.
In Most of the Cases We Reviewed, Foster Youth Had Received Needed Services Only After Significant Delays
State law grants foster youth the right to access and receive medical, dental, vision, mental health, and substance use disorder services and reproductive and sexual health care with reasonable promptness that meets the needs of the youth. With respect to the medical and mental health needs of foster youth, the Legislature has pursued ensuring this access through mechanisms that include the interagency MOU intended to facilitate timely, trauma‑informed services for foster youth; the implementation of a program that requires counties to use foster care public health nurses to marshal medical, dental, and mental health information and coordinate care for foster youth; and through individual case plans that are intended to ensure proper care and address the needs of youth while they are in foster care. Therefore, as an entity that participates in and administers these mechanisms, it is reasonable to expect that the department would engage in sufficient efforts to ensure that the youth in its care access necessary services in a timely manner.
However, the department did not always ensure timely provision of services for some of the youth whose cases we reviewed. To the extent that the department had documentation related to the timeliness of services provided to foster youth, we reviewed whether the department provided those services directly or through its interagency partners within the specified timelines or frequencies. As we discussed earlier, our review of the 125 services that 36 youth needed to receive found that the department had available documentation related to only 60 services to demonstrate whether youth received those services within the expected time frames or frequencies. Our review of these 60 services found that 27 services were not provided in a timely manner, as Table 3 shows. Although the department generally ensured that youth received timely services related to transitional housing and education supportive services, it did not ensure timely health, dental, sexual education, and independent living services for many of the youth whose cases we reviewed.
Health and dental services are the most common services youth receive. However, the department did not ensure that all youth received them within the designated time frames. For example, both a physical exam and a dental exam are required within 30 days from the removal of youth from their home. However, the department did not ensure that any of the 13 youth for whom we selected dental services and whose case files contained necessary documentation received the required dental exam within 30 days. For example, one such youth had a removal date of September 14, 2018, but the first documented mention of a dental exam was not until November 4, 2019. In fact, the average delay in providing the initial dental exams for our selected 13 case files was 318 days, or more than 10 months. Similarly, health services for 11 of the 28 youth whose case files we reviewed and that included the necessary documentation had an average delay of 85 days.
In some instances where documentation existed, the department noted that causes for delay included that the youth was missing from care or the caretaker had difficulty securing an appointment. Missing from care refers to youth who are absent from their respective placement without permission. For example, youth who run away from their foster home are considered missing from care. A case file we reviewed for one youth indicated that the youth was missing from care and therefore, did not attend a scheduled appointment. However, the department did not document the cause of 23 of the 27 documented delays we identified. Although the department was not aware of the specific reasons for delays with these services, a management analyst at the department stated that a number of factors may contribute to delays in health or dental appointments that may or may not be documented. Dental services for youth may be delayed, for example, because of the youth’s fear of dental appointments. Routine health services, by contrast, may be delayed for older youth because they may not perceive a need to go to the doctor. The management analyst agreed that child welfare workers should document the causes of such delays.
Without fully understanding the reasons for delayed services, the department cannot take the necessary steps to make improvements and ensure that all youth receive timely services, which can negatively affect the health and well‑being of the youth in its care. According to the U.S. Department of Health and Human Services, children in foster care are particularly likely to have had multiple types of adverse experiences that increase the risk of serious health conditions or negative health outcomes. Timely services are necessary to ensure that the department can sufficiently address the needs of these youth. For example, a youth with a mental health diagnosis may require prescription medication, and services delivered late may make it difficult to ensure effective medication management and compliance. Even though the causes of delayed service delivery may sometimes be beyond the department’s control, such as when a youth is missing from care, the department must make sufficient efforts to ensure that all youth receive timely services. However, the department cannot do so without understanding the reasons for delayed services.
The Department’s Efforts to Connect Youth With Family and Keep Them Safe in Temporary Shelter Have Been Inadequate
Key Points
- State law requires the department to identify, locate, and notify all relatives as potential caretakers for youth; however, in five cases we reviewed the department could not demonstrate that it took these steps. Known as family finding and engagement, these steps are critical because they aim to build permanent, caring relationships for youth with family members and supportive adults. Because the department lacks evidence of its efforts to identify relatives and other potential caretakers, it lacks assurance that its staff have taken sufficient steps to identify all possible options capable of providing stable, permanent placement or ongoing support for the youth.
- While awaiting a stable placement with family members or other potential caretakers, youth at Alameda County were often placed in the county’s transitional shelter. Although not currently operational, this shelter provided temporary housing—not to exceed 72 hours—and supportive services to youth. While it was operating, youth in the shelter may have faced safety risks in large part because the department faced challenges with minimizing the time youth spent in the transitional shelter, where some youth were absent from their respective placement without permission.
The Department Has Not Prioritized Efforts to Ensure That Foster Youth Connect With Family
Family Finding and Engagement is a framework that includes efforts to nurture life‑long familial connections for youth in foster care, and it also represents statutory requirements to identify, locate, and notify relatives of a youth in foster care, as the text box describes. State law requires that all foster youth have the right to live in a safe, healthy, comfortable home where they are treated with respect. These rights include placement with a relative, if an appropriate and willing individual is available. Therefore, after a court orders the removal of a child from the custody of a caretaker for reasons necessary to protect the child, state law requires the department to conduct an investigation within 30 days to identify, locate, and notify all relatives about the various options they may have to provide support or possibly act as a caretaker for the foster youth.10
Family Finding and Engagement Is a Broad Concept That Involves the Following:
Family Finding: Investigation to identify and connect the youth, who may be disconnected from parents, with kin to provide family support and possible placement.
Engagement: Nurturing engagement and support by potential permanent connections with multiple family members, not only the primary caretaker, so they can become part of a permanent support network for the youth. Developing connections includes activities and interactions that create effective relationships between the youth, caregiver, and extended family, which are critical for the youth’s well‑being, especially when placed with non‑relative caretakers.
Source: State Law and CDSS’s All County Letter.
The Department Could Not Always Demonstrate Its Family Finding Efforts
In all five cases we reviewed, the department could not demonstrate the efforts it made to identify, locate, and notify relatives of foster youth in care.11 We expected the department to document its efforts, such as asking the youth about their relatives and contacting all identified relatives by telephone, email, or through in‑person visits. However, hard copy and electronic case files records and the department’s reports to the court did not include substantive information about the efforts its staff took to identify, locate, and notify all relatives as potential support or caretakers. Available documents also did not clearly indicate whether the court agreed that the department conducted a thorough investigation to identify and notify all possible relatives in four of the five cases. The department acknowledged that it lacks specific policies or procedures to ensure its staff comply with family finding and engagement requirements within 30 days of a youth’s removal from their homes. However, the department stated that it expects to implement a policy by the end of September 2025.
Further, although the department has a policy requiring staff to take specific steps to identify relatives, we did not find evidence that it took such steps. Specifically, the department has a policy that requires child welfare workers to ask participants, such as the youth and parents, when they meet in a Child and Family Team (CFT) meeting—which identifies support and services that are needed to achieve permanency, enable a youth to live in the least restrictive family setting, and promote normal childhood experiences—to identify relatives for potential placement or support. CDSS, in a letter sent to all counties, required the department to conduct CFT meetings at a minimum of every six months to identify support and services that a youth needs to achieve permanency, to enable a youth to live in the least restrictive family setting, and to promote normal childhood experiences. We reviewed 44 CFT meeting action plans and summary documents related to all cases we selected, and found that records for only 23 percent of the CFT meetings noted discussion about a youth’s placement with relatives, and about 11 percent noted discussion about relatives providing support to the youth.
Department staff noted that the department’s record of placing youth with relatives or non‑relative extended family members is higher than the state average. According to the California Child Welfare Indicator Project (CCWIP),12 from 2019 through 2024, Alameda County made a first placement for an average of 36 percent of foster youth with relatives or non‑relative extended family members, which is three percentage points higher than the state average of 33 percent. Although the department’s first placement of foster youth is higher than the state average, without formalized policies and training that ensure consistent, accurate, ongoing, and legally required investigations to identify, locate, and notify relatives, the department risks overlooking appropriate relatives for a youth’s placement who could potentially provide a stable, supportive environment.
The Department Did Not Always Make Efforts to Identify and Engage All Family Members
We also found that the department did not always continue its family finding and engagement efforts to find all family members. Until the court determines the youth’s permanent placement, state law requires the department to report on the status of the youth’s placement in foster care at least every six months. For this review, the department must show that the youth’s placement is still necessary and appropriate, meaning that it serves the youth’s best interests, including special physical, psychological, educational, medical, or emotional needs. For example, to preserve and strengthen a youth’s family ties whenever possible, if a relative requests placement of the youth, the department must give preferential consideration to placing the youth with that relative, if appropriate. As of January 2025, state law also requires the department to document whether it has made continued efforts—and the outcomes of those efforts—to locate relatives if the youth is not residing with a relative. According to CCWIP data, from 2019 through 2024, Alameda County placed an average of 44 percent of foster youth with relatives or non‑relative extended family members as the youth’s main placement for more than half the days spent in foster care, which is four percentage points lower than the state average of 48 percent.
We reviewed 10 cases and found that in five of them, the department’s reports to the court indicated that there were no known potential caretakers for the youth. However, these reports did not include information about the efforts the department made to search for relatives as potential caretakers. For instance, in its reporting on one case, the department described an older youth who was placed in a foster family agency home. The report identified an older sibling and paternal grandmother as part of the youth’s support network, but those reports do not demonstrate whether the department determined if these relatives were willing or appropriate for the youth’s placement.
Further, the department did not perform continued family engagement to expand the youth’s family network. Beyond requirements to identify, locate, and notify relatives for possible placement, family finding and engagement focuses on building a permanent network of connections to support the youth throughout their life. These efforts start with finding relatives and should include ongoing follow‑up and engagement to ensure not only that the youth resides with the ideal caregiver, but it should also ensure that the youth has the opportunity to develop and maintain other relationships that could serve as life‑long familial support. In five of the 10 cases, the department’s reports do not provide information about the efforts it made to determine whether any identified relative would be an appropriate provider of support for the youth. As Figure 9 shows, for a youth who had been in the foster care system for more than two years and received placement and support from several different relatives, the reports do not demonstrate that the department made efforts to contact seven other identified relatives. Without evidence that the department provided ongoing family finding and engagement efforts, the department cannot be sure that it did not miss opportunities to identify additional relatives who could have provided stable, permanent placement or ongoing support for the youth.
Figure 9
The Department Does Not Generally Perform Continued Family Engagement to Expand the Youth’s Family Network

Source: Auditor review of case files on the department’s CWS/CMS.
Figure 9 is an infographic describing that the department does not generally perform continued family engagement to expand the youth’s family network. The Figure describes two scenarios based on review of department casefiles. Scenario one described that for a youth in foster care for more than two years, the court determined to stop reunification services between the youth and parents, and appropriate relatives willing to provide permanent placement for the youth, such as by adoption or guardianship were not identified. The department completed a Family Finding and Engagement report that identified 11 potential relationships or sources of information that could assist in locating relatives for permanency support and placement assessment. In the span of five years, the youth experienced placements with two different relatives and regularly communicated with three other relatives. The department’s reports to the court do not include information that it made efforts to contact seven other identified potential connections who may have been able to provide permanent placement. Scenario two described that for an older youth in foster care, the court determined to remove the youth from the parents’ custody in late 2022 and placed them in a Foster Family Agency home. The department’s reports to the court, from April 2023 through February 2025, indicate at least two people most important to the foster youth are their siblings. The youth had occasional contact on social media with their siblings, which the foster caretaker facilitated. Reports from September 2024 and February 2025 indicate that the youth had an in-person visit with siblings during each reporting period. The source of the Figure is auditor’s review of case files on the department’s CWS/CMS.
The department explained that it does not have a sufficient number of child welfare workers to conduct intensive family finding efforts for every foster youth. Currently, the department has one child welfare worker dedicated to intensive family finding efforts for foster youth up to age 6 or when the child welfare workers assigned to cases are unable to identify relatives. The department has an agreement with Casey Family Programs to provide, among other things, case management services in an effort to promptly achieve a stable, permanent placement for foster youth ages 11 through 18.13 The department said it requires supervisors to facilitate CFT meetings and interview youth to solicit information and identify relatives for potential placement or to provide support to the youth. However, as we described previously here and also previously here, our review found that most of the cases we reviewed did not include discussion about a youth’s placement with relatives and about relatives providing support to the youth. Unless the department consistently identifies all relatives and regularly determines whether they are willing and suitable to provide placement or support for a youth, the department may not recognize opportunities for stable, permanent placement or ongoing support.
The Department Did Not Ensure that Youth Maintained Sibling Relationships
Because a youth’s well‑being is related to their relationships with people who are significant in their lives, the law is designed to preserve and strengthen a child’s family ties—including sibling relationships—whenever possible. For foster youth with siblings, state law requires the department to make a diligent effort to develop or maintain the sibling relationship and to place siblings together or to develop a visitation plan when the court determines that such efforts are appropriate.
The department fell short in its efforts to fulfill state requirements and to support and maintain sibling relationships. In our review of the selected 10 cases, we found that in four cases for foster youth who had one or more siblings, there were periods during which the youth had little or no contact with their siblings. In one of these cases, the department’s reports to the court indicate that at least two of the people most important to the foster youth were their siblings. The youth had occasional contact on social media with those siblings, which the foster caretaker facilitated. The report also noted concerns that the youth felt sad and lonely, had limited contact with relatives, and, as a result, sometimes left the foster home without permission. However, the reports do not include information that the department made efforts to develop or maintain the sibling relationship for this youth, as scenario 2 in Figure 9 shows. When a child in foster care has a sibling but is not placed with them, the department acknowledges the need to improve its documentation. This includes recording both the reasons for not placing siblings together and the reasons it is not making efforts to develop and maintain the sibling relationship or to develop visitation plans, such as when doing so conflicts with the child’s safety or well‑being. The department also recognizes that mistakes can occur, and in some cases, it may fail to make these efforts without providing a reason. However, it does not believe that its failure to act is the primary cause of lack of sibling relationship and visitation.
The Department’s Plans May Not Fully Address Gaps in Its Family Finding and Engagement
The department plans to expand its family finding and engagement policy. It said that several factors led to expanding its family finding and engagement since early 2024. In 2023, CDSS notified all counties that it had contracted with the University of California, Davis to launch the Center for Excellence (CFE) in Family Finding, Engagement and Support to support county child welfare agency efforts to keep youth connected to their relatives. The department recognized an opportunity to expand its family finding and engagement efforts and in 2024 opted to join the Kin‑First Accelerator Program, led by the CFE and partners. The program is designed to prioritize kinship care to create more supportive and stable environments for youth in the child welfare system, aligning with the overarching goal of improving child welfare outcomes statewide. In February 2025, CDSS allocated more than $2.5 million to the department for specialized permanency services and support to supplement existing funding for family finding and engagement programs.
In 2024, the department published a County Self‑Assessment for 2018 through 2023 in response to a state law requirement under the California Child and Family Services Review System. Based on the self‑assessment, the department then developed a five‑year System Improvement Plan (plan) for 2024 through 2029. One of the strategies in the plan states that the department will enhance the use of family finding and engagement resources at key points in the timeline of its efforts to achieve a permanent, stable living situation for a foster youth. These efforts begin, for example, when a youth enters foster care, and then continue throughout the case lifecycle when the department revisits family finding and engagement efforts at key permanency decision points for the youth. Specifically, the department’s plan includes partnering with Casey Family Programs to provide family finding and engagement services to youth with few or no identified relatives and for youth ages 14 through 21. The plan also includes the development of a scope of work to contract with a provider for additional family finding and engagement services for children up to 21 years old. However, the department’s plan does not include strategies for enhancing the department’s efforts for maintaining sibling interactions and relationships.
In the Absence of Stable Placement Options, the Department Had Housed Many Youth at Its Former Transitional Shelter Where Youth May Have Faced Safety Risks
Although state law grants youth the right to be placed in a safe, healthy, and comfortable home where they are treated with respect, it is not always possible for the department to immediately identify a suitable placement option when youth are removed from their homes. In some cases, a transitional shelter can serve as a temporary placement for youth before the department locates placement with family, foster family, or another emergency housing provider. The Joint Legislative Audit Committee (Audit Committee) requested that we review the department’s approach to ensuring the health and safety of youth placed in the transitional shelter. The department operated a transitional shelter until July 2024 during our review period. The transitional shelter’s license with CDSS allowed it to provide pre‑admission medical and mental health screenings, and temporary care for up to 30 youth at a time, for a maximum of 72 hours while youth await stable placement. Further, the shelter is only meant to serve as a temporary placement and the youth can enter and leave the shelter at will. The department says that it suspended all operations at the transitional shelter in July 2024 for several reasons, including a complaint by the city of Hayward in which it was located. The department plans to reopen a transitional shelter at a new location, but it has not yet determined an opening date. WestCoast Children’s Clinic (WCCC), the same nonprofit children’s psychology clinic that Alameda County contracted with to manage the day‑to‑day services at the now‑closed transitional shelter, will manage the county’s future transitional shelter. Although WCCC provides ongoing management and staffing, the department, as the license holder for the transitional shelter, remains responsible for maintenance and oversight of the shelter.
CDSS has established requirements for licensed community care facilities, such as the transitional shelter, to ensure the health and safety of youth placed in those facilities. For example, CDSS standards require license holders to conduct criminal record reviews of all employees and to safely store medications. Further, CDSS standards require specific indoor and outdoor spaces and specific staff to youth ratios, as Figure 10 describes. To ensure that these facilities comply with standards and provide the expected quality of care, CDSS may inspect licensed community care facilities as it deems necessary. Regulations require CDSS to issue reports on any deficiencies it finds because of these inspections. We reviewed 18 inspection reports that CDSS prepared for Alameda County’s transitional shelter from fiscal years 2020–21 through 2023–24, and four of these 18 reports identified deficiencies related to the department’s late reporting of critical incidents or submitting reports without adequate details. This type of deficiency could compromise CDSS’s ability to monitor these incidents at a transitional shelter in a timely manner.
Figure 10
CDSS Establishes Safety Requirements for Transitional Shelters
Source: CDSS’s County Transitional Shelter Care Facility Operating Standards.
Note: This graphic represents a hypothetical facility and does not reflect the actual setup of the department’s transitional shelter.
Figure 10 is a cutaway of a house representing a transitional shelter that describes the safety requirements that the California Department of Social Services established. Above the cutaway, there is a list of selected staff requirements: 1. All staff must have criminal record clearances. 2. There must be one staff member per six youth aged 7–18. 3. All childcare staff must complete 20 hours of training annually. Within the cutaway, there are abstract images of youth and the furnishings of the facility. The figure lists the different safety requirements for a transitional care facility: emergency intervention, facilities will use emergency interventions to prevent a youth who exhibits assaultive behavior from injuring or endangering themselves or others; no more than two youth shall sleep in one room; youth of the opposite sex shall generally not share a bedroom unless they are siblings or under age 5; faucets used for grooming should be deliver hot water, and all toilets and bathing facilities shall be maintained in good condition; youth shall have access to safe outdoor activity space. The Figure notes that the graphic represents a hypothetical facility and does not reflect the actual setup of the department’s transitional shelter. The source of the Figure is CDSS’s county transitional shelter care facility operating standards.
All community care facilities, such as Alameda County’s transitional shelter, must report critical incidents to CDSS according to a defined schedule. Facilities must report in writing within one working day of normal business hours any critical incident, including a youth’s death, injuries that require medical attention, or instances in which youth are absent from their respective placement without permission and their safety is at risk. Facilities must submit reports of certain other incidents, such as those in which a youth assaults another person at the facility or incidents in which a youth is detained in a juvenile institution, within seven days.
CDSS’s evaluations found that the department did not submit critical incident reports in a timely manner or that the reports were not thorough enough. For example, in one instance in March 2024, CDSS found that the department submitted multiple critical incident reports from November 2023 after the 7‑day requirement. In October of 2023, CDSS found that the department submitted incomplete critical incident reports, such as reports that lacked the strategies used to redirect youth from leaving the transitional shelter and police report numbers from when youth did leave the shelter. In response to deficiencies that CDSS found in 2023, the department stated that transitional shelter staff received training on how to report critical incidents. Nonetheless, CDSS found similar issues with critical incident reporting the following year because the department could not demonstrate that it resolved all of its deficiencies. Given that CDSS is the oversight entity to ensure license holders have adequate processes in place to safeguard the health and safety of youth at the transitional shelter, lack of reporting timely updates to CDSS about critical incidents at the transitional shelter may prevent CDSS from promptly intervening to ensure youth’s safety, when needed.
We reviewed the transitional shelter’s critical incidents that it reported to CDSS from August 2020 through December 2024 and found that some youth who were staying at the transitional shelter were involved in critical incidents while missing from care, putting their health and safety at risk. As we described previously, missing from care refers to youth who are absent from their respective placement without permission. The transitional shelter manager stated that staff attempt to use many different tactics to encourage youth to stay at the transitional shelter, including conversations, ordering a youth’s favorite food, and providing youth opportunities to have their hair styled. However, these strategies do not always work. To monitor the entry and exit of youth at the transitional shelter, the department contracted with a security firm. However, such security personnel cannot prevent youth from leaving the transitional shelter without authorization. State law prohibits the department from locking foster youth in foster care placements unless the placement is in a community treatment facility.
Our review of 166 critical incidents that the department reported to CDSS from January 2020 through July 2024 found that the most prevalent critical incidents included youth who threatened to assault another youth or a staff member, as Figure 11 shows. Our review of critical incident reports also found that youth who were missing from care were often involved in incidents like drug or alcohol use. The department’s entry and exit data show that 22 to 57 percent of youth entries at the transitional shelter each year were missing from care at some point, as Table 4 demonstrates. In addition, our review of 28 critical incident reports related to youth missing from care found that at least 14 youth were involved in such incidents. We found that in eight instances, youth returned to the transitional shelter under the influence of drugs, and in two instances youth reported having experienced sexual assault while away from the transitional shelter.
Figure 11
The Most Common Critical Incidents the Department Reported Involved Threats to Youth and Staff, January 2020 Through July 2024
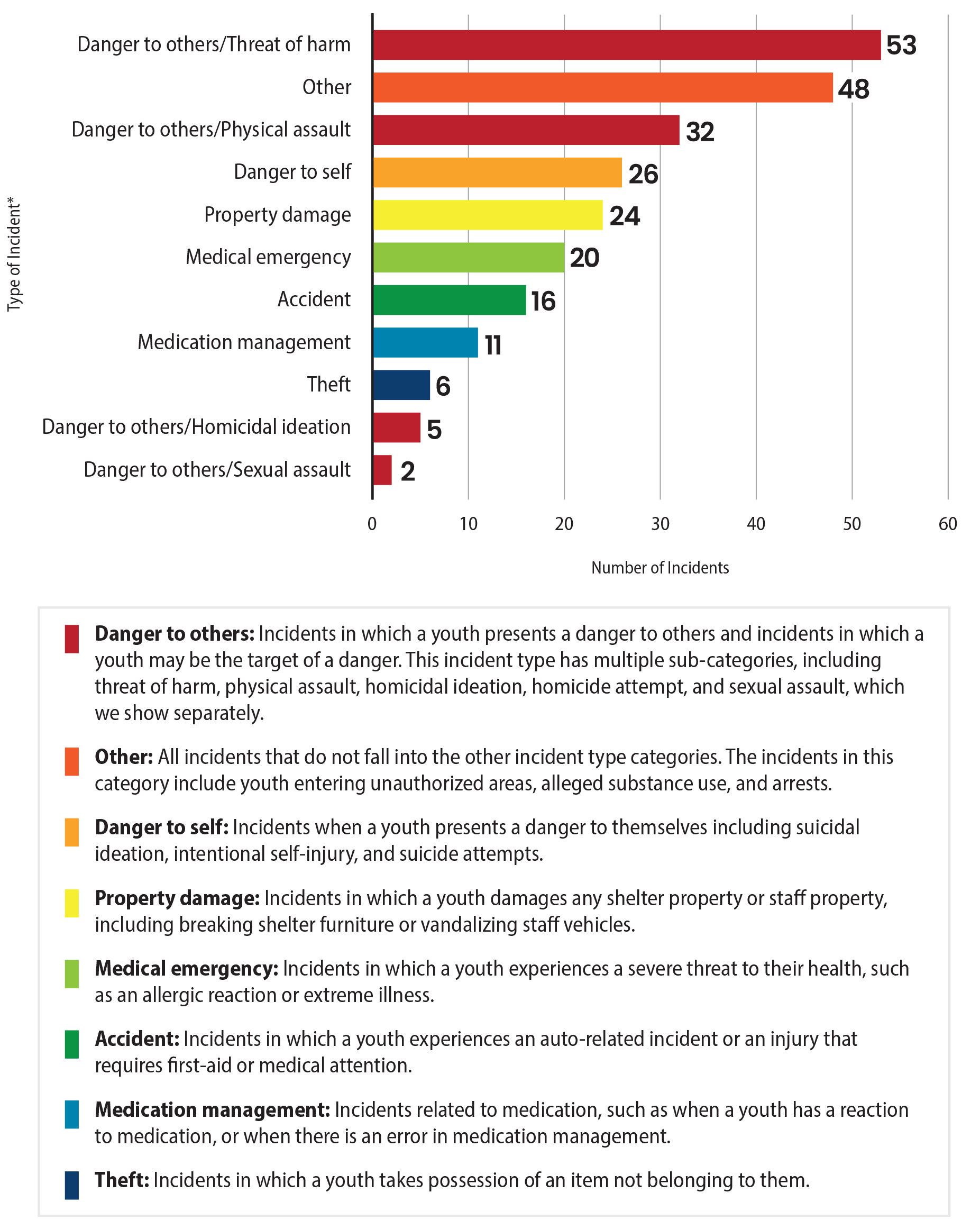
Source: Review of critical incident reports.
Note: The department did not begin to track the Theft category until August of 2021.
* The department reported a total of 166 critical incidents to CDSS from January 2020 through July 2024. However, some incidents involved more than one type of incident.
Figure 11 is a bar chart describing the number of the most common critical incidents the department reported involving youth in its transitional shelter from January 2020 through July 2024. The graphic lists the types of incidents in descending order of frequency. The bottom half of the figure contains more detailed descriptions of the incident types. Danger to others is an incident type in which a youth presents a danger to others and incidents in which a youth may be the target of a danger. This incident type has multiple sub-categories, including 53 incidents of a threat of harm, 32 incidents of physical assault, 5 incidents of homicidal ideation, and two incidents of sexual assault. Other is an incident type representing 48 incidents that do not fall into the other incident type categories. Danger to self is an incident type that includes 26 incidents in which a youth presents a danger to themselves including suicidal ideation, intentional self-injury, and suicide attempts. Property damage is an incident type accounting for 24 incidents where a youth damages any shelter property or staff property including breaking shelter furniture or vandalizing staff vehicles. Medical emergencies are an incident type representing 20 incidents in which a youth experiences a severe threat to their health, such as an allergic reaction or extreme illness. An accident is an incident type that includes 16 incidents in which a youth experiences an auto-related incident or an injury that requires first-aid or medical attention. Medication management is an incident type representing 11 incidents related to medication, such as when a youth has a reaction to medication, or when there is an error in medication management. Theft is an incident type including six incidents in which a youth takes possession of an item not belonging to them. The department reported a total of 166 critical incidents to CDSS from January 2020 through July 2024. However, some incidents involved more than one type of incident. The Figure notes that the department did not begin to track the Theftcategory until August of 2021. The source of the Figure is a review of critical incident reports.
CDSS’s annual inspection reports also discussed issues related to reducing the number of youth who stay longer than 72 hours at the transitional shelter, emphasizing the need to rely less on the transitional shelter and ensure that youth have stable placement options. We reviewed the department’s transitional shelter entry and exit logs from calendar years 2019 through 2024 and found that many youth stayed at the transitional shelter longer than the 72‑hour limit, increasing the likelihood of them getting into a critical incident while in the transitional shelter’s care. In fact, in our review of transitional shelter logs for the six years of our review period, we determined that the department housed an average of 17 percent of youth at the transitional shelter for longer than the 72‑hour limit. As Table 5 shows, the average length of stay for those who exceeded 72 hours was 139 hours, nearly double the limit.
Our review of a selection of 30 case files for youth who stayed at the transitional shelter for more than 72 hours from January 2019 through July 2024 found that in 17 cases, the department cited that placement options were few or difficult to find because of the behavioral, physical, and emotional needs of the youth. For example, the department’s entry log notes that one youth with autism stayed at the transitional shelter for 200 hours, citing that there were no homes to meet the child’s needs before the 72‑hour limit. According to the transitional shelter’s division director, finding providers to accept placement for youth with complex behavioral needs is more difficult, and the number of providers who can provide adequate care for youth with complex needs has decreased over the years. The department also explained that youth can overstay for other reasons. The department’s division director for the transitional shelter said that if, for example, a youth needs a Short Term Residential Therapeutic Placement (STRTP), it can take longer than 72 hours for the STRTP staff to acknowledge the referral. Then, it can take as long as five days from the youth’s arrival at the STRTP for the program to determine whether it will accept the existing mental health assessment or whether conducting a new assessment would be more clinically appropriate. The division director for the transitional shelter also stated that housing providers may not accept youth with placement failure histories, youth with substance abuse issues, or youth who refuse to attend school.
Although the department discussed with CDSS strategies to minimize overstays, as some transitional shelter evaluation reports from 2021 to 2023 documented, the department did not have formal policies or processes to track and minimize overstays. The assistant agency director and transitional shelter division director stated that, although the department has strategies to minimize overstays, it is open to formalizing these processes for the new transitional shelter. Until the department formalizes a process to minimize overstays, it will not be able to ensure that its staff are exhausting all strategies to reduce the time a youth is at the new transitional shelter and, therefore, it will not be able to reduce the likelihood of youth being involved in potential critical incidents, such as injuries or assaults, while staying at the transitional shelter.
Although the department has taken some steps to prevent overstays and critical incidents in the future, it needs to track and assess data related to incidents at the transitional shelter to better inform its processes. The department has developed new draft emergency intervention policies for its future transitional shelter and reduced the capacity of the new 72‑hour shelter to serve only 10 youth at a time compared to 30 in the previous shelter. Additionally, according to department staff, the new transitional shelter will consist of two buildings and will be in a quiet, rural community with a large outdoor space and a gate. It will also have minimal access to public transportation, which could make it difficult for youth who try to run away from the shelter. Despite these efforts to prevent youth from leaving the planned transitional shelter, the department’s plan does not include tracking trends in critical incidents, which is a practice that CDSS recommends, at the planned shelter. Without identifying high‑level trends in critical incidents, the department may be unable to identify possible incident prevention measures that could better ensure the safety of youth at the new transitional shelter. After we brought this shortcoming to the department’s attention, it acknowledged that it should track trends in critical incidents.
Further, as a best practice, we expected the department to periodically perform self‑evaluations of the previous shelter’s performance and to have policies and procedures to do so; however, it did not. Although not a requirement, a CDSS best practice is to ensure continuous quality improvement. Best practices from other government entities suggest that periodic performance assessments could provide the department with opportunities to strengthen its operations by identifying any issues and opportunities to correct them as soon as possible. We reviewed the department’s transitional shelter policies for the new shelter and found that the department neither periodically self‑evaluates transitional shelter performance, nor does it have any internal policy or procedure for evaluating transitional shelter performance or documenting corrective action for identified issues. The assistant agency director agreed that the new transitional shelter should develop and implement such policies. Without such policies, the department could miss the opportunity to identify deficiencies before they require CDSS’s intervention.
Other Areas We Reviewed
To address the audit objectives approved by the Audit Committee, we also reviewed the following:
- Whether the department has had a training program to ensure that employees are aware of departmental case processing standards and best practices, including identifying the number of employees who have received training and how often such training has occurred.
- Whether the county has had sufficient processes for cross‑collaboration with other agencies and entities as state law requires, including its adherence to the MOU’s required process for youth with complex needs.
The Number of Child Welfare Workers and Supervisors Who Have Not Completed Required Core and Continuing Trainings Has Increased Over the Past Five Years
Both a 2003 Federal Child and Family Services Review and the resulting Program Improvement Plan required the development and implementation of statewide, standardized core curricula for child welfare workers and supervisors. Accordingly, CDSS implemented its core curricula, known as the California Common Core Curricula, in 2017 and revised the training time frame requirements in July 2021. This curricula ensure that all new child welfare workers receive the foundational training necessary for their work and that all supervisors receive training in the core skills required to lead and supervise their units.
Newly hired child welfare workers receive core training on topics such as trauma‑informed practice, knowledge of state and federal laws, and introduction to child development and the CWS/CMS system. Newly hired, assigned, or promoted supervisors who directly manage staff receive core training on topics such as case work supervision; managing results and supervising to achieve outcomes, including compliance with state and federal reporting requirements; and other essential topics, as the text box describes.
Child Welfare Worker Core Training Includes:
- Orientation to California Child Welfare Practice
- Introduction to Child Development
- Trauma‑Informed Practice
- Fairness and Equity
- Child and Family Teaming
- Federal and State Laws
- Legal Procedures and Responsibilities
- Introduction to Indian Child Welfare Act (ICWA)
- ICWA and Working with Native American Families & Tribes
- Key Issues in Child Welfare: Behavioral Health, Substance Use Disorders & Intimate Partner Violence
- Key Issues in Child Welfare: Social Worker as Practitioner
- Introduction to CWS/CMS
Supervisor Core Training Includes:
- Promising and research informed practice
- Educational supervision
- Policy context for child welfare practice
- Managing results and supervising to achieve outcomes, including compliance with state and federal reporting requirements
- Case work supervision
- Fiscal fundamentals for children’s services
Source: Review of California Social Work Education Center Curriculum and CDSS’s Manual of Policies and Procedures for Staffing Development and Training.
From February 2017 through June 2021, CDSS required staff to complete their core training within 12 months from the date of hire, assignment, or promotion. However, beginning July 1, 2021, CDSS only recommended that staff complete their core training within the same 12‑month period. After completing their core training, all child welfare workers and supervisors must complete 20 hours of continued training annually. Additionally, state law requires the department to report to CDSS at least once each year on several training topics, and among such topics are the number of county child welfare workers and supervisors who received training and the types of training.
From fiscal years 2019–20 through 2023–24, the percentage of child welfare workers and supervisors who did not complete the required core and continuing training increased, as Table 6 shows. According to the department’s training and consulting team staff development manager, issues of workload, scheduling conflicts, and absences are the reasons staff did not complete their core and continuing training. The intent of the statewide, coordinated training program is to provide practice‑relevant training that addresses critical issues affecting the well‑being of youth. Because the department has not consistently ensured that its child welfare workers and supervisors complete this training, it cannot be certain that it is doing everything possible to protect the health and safety of youth and families in Alameda County.
The department has not taken all the steps it can to ensure that staff complete the required training. The department’s Training Unit indicated that it uses a Learning Management System to track and monitor the completion of required core training by child welfare workers and supervisors. The Training Unit first enrolls all child welfare workers and supervisors into their core training courses. If a worker or supervisor does not complete the required core training within a designated time frame, the Training Unit will schedule the worker for the next available training session or for a session that fits the supervisor’s schedule. However, the Training Unit said that it has not established a process to monitor the completion of ongoing annual training by staff. According to the department’s training and consulting team staff development manager, in March 2025, the Training Unit submitted a report to the department’s executive team and division directors identifying child welfare workers and supervisors who had not completed their required 20 hours of annual continuing training. Starting in January 2026, the Training Unit intends to send this noncompliance report to the executive team and division directors annually.
Service Provider Contracts Frequently Lack Performance Metrics for Timeliness of Services, Which Has Hindered the Department’s Ability to Hold Providers Accountable
For services that the department cannot provide through its MOU partners—such as support services for youth who have experienced commercial sexual exploitation, youth employment programs, and emergency housing—the department contracts with third‑party service providers. To improve service delivery that results from such contracts, the department directed staff to implement results‑based accountability (RBA) measures in its contracts starting in 2017. The goal of these metrics is to measure the number of people the contract served, how well the contractor performed its duties, and the number of youth who demonstrate improvement after the provision of services. We reviewed the department’s 38 contracts that provided services to youth as part of the foster care program from fiscal years 2019–20 through 2023–24. Only seven—two contracts for short‑term residential programs and emergency shelters and five contracts for various youth support programs—included timelines and performance metrics. The remaining 31 contracts did not include timelines or performance metrics related to the timely provision of services, as Table 7 shows.
The RBA framework asks three questions to develop metrics, including how well the contractor completed the work. In asking how well the contractor completed the work, the RBA model metric can consider timeliness as one of several quality metrics. Other metrics considered include the percentage of clients who completed an activity, the percentage who met a given standard, and the percentage of contract activities that clients completed correctly. As Table 7 shows, the department included timeliness metrics for some of its contracts. For example, two contracts for the transitional housing program—part of youth support programs—require that 75 percent of participants meet once per week with a youth advocate. Another contract for a short‑term residential program requires that 90 percent of its referred participants receive assessments within three to 30 days, depending on the priority of the referral. Further, the contract requires that 90 percent of referred participants have follow‑up services scheduled within 15 days of assessment. While it may be necessary to modify time frames and performance metrics for specific services, we would expect all contracts to include time frames and metrics to ensure that youth receive services in a timely manner.
Lack of time frames for delivery of contracted services and related performance metrics may keep the department from ensuring that they are delivered to youth timely and as expected. As we discussed earlier in Table 3, we reviewed five instances of Independent Living Program Services, which the department provides through contractors. In two of those cases, the first documented instance of the services were delayed. We found that the contracts for providers involved in these cases did not include time frames or performance metrics related to timeliness. Although contractors may have valid reasons for not meeting timeliness metrics, including such metrics would enable the department to hold contractors accountable for timely services.
According to a senior analyst for the department, not all contracts contain metrics specific to the timely delivery of services because, depending on the service, other performance metrics may be more significant to ensure the adequate delivery of services. For example, the analyst explained that a contract for legal services for youth contains a metric for the number of referred youth served rather than for timeliness because a short time between referral and delivery of legal services would not impact whether the youth received adequate legal services. She further explained that even though a contract does not include a performance metric for timely delivery, the department is able to ensure that timely delivery of services occurs. According to the department, contract managers consider timeliness in their oversight of contracts and, if they believe services are not provided with sufficient timeliness, department staff will work with contractors to determine and improve causes of delayed services. However, even for those contracts that include time frames for the delivery of services, they do not always include a performance metric to track whether the contractor follows that time frame. For example, a contract for a youth employment program has a time frame for intake, enrollment, and job readiness training, but the contract does not contain a metric to track how many youth received services according to that time frame.
The internal communication that outlines the requirement to include RBA measures in contracts starting in 2017 does not specify a deadline by which all existing contracts between the department and its contractors should have RBA performance metrics, limiting the department’s ability to hold contractors accountable for timely delivery of services. According to department staff, the effort to add RBA measures to all contracts is ongoing. Although child abuse prevention contracts have similar time frames, other contracts require the development of service‑specific time frames. Specifically, child abuse prevention contracts require intake within one week of referral and an assessment within one week of intake. However, we observed that most of these contracts do not specify the number of youth the contractor should serve within a specified time frame. Further, youth employment program contracts are inconsistent in their time frames. For example, one contract for a youth employment program requires one month to complete screening, application, intake, and interview with case manager; two weeks for enrollment and assessment; two weeks to develop an action plan with a career counselor; and one month of job readiness training. However, four other contracts for youth employment programs do not have time frames for service delivery. The department generally agreed that having performance metrics for timeliness in its contracts would ensure better provision of services to foster youth.
Recommendations
Alameda County Department of Children and Family Services
To ensure that it timely initiates and completes investigations of all immediate and non‑immediate referrals, the department should, by January 2026:
- Ensure that all supervisors review and approve investigation reports in a timely manner to ensure that they agree with the disposition.
- Periodically review the status of all referrals to determine the number of days to initiate and complete investigations and work with staff to identify impediments to initiating and completing investigations within the required time.
- Develop a strategy to address all identified impediments to ensure that it reduces the number of days for initiating and completing all investigations to comply with required time frames.
To ensure that it has sufficient staff to provide timely investigations of child abuse and neglect referrals and the timely provision of foster care services, the department should do the following by October 2026:
- Survey all staff to identify impediments to retention and recruitment of staff and develop an action plan to address the identified impediments.
- Hire more staff in the CWW I classification, up to 50 percent of the total child welfare workers in the department’s ER Unit, as CDSS allows.
- Make its shadowing process mandatory for new employees to reduce the time supervisors spend training new staff.
To ensure that foster youth receive all necessary services within the prescribed or agreed‑upon time frames, the department should create and implement policies and processes that include the following by October 2026:
- Documenting the service referral dates for all services.
- Documenting all service provision, including dates when a service was provided to foster youth through an interagency partner or a contractor.
- Reviewing and documenting, at least monthly during their visits with youth, whether youth receive services according to agreed‑upon time frames and frequencies.
- Documenting all efforts to collaborate with interagency partners to ensure timely service delivery, including efforts to obtain documentation of needed services, time frames, and delivered services.
To ensure that it has the necessary documentation to identify all services that partner agencies provide to youth and to ensure the timeliness of those services, the department should propose a change to the MOU to provide for information sharing. This information should include the types of services that youth are scheduled to receive, the dates the youth were referred for services, and when the services were provided to ensure timely and coordinated delivery of services.
To ensure that the department’s child welfare workers consistently and accurately identify, locate, and notify all possible relatives of a youth within 30 days of the youth’s removal from a caretaker, the department should develop policies and procedures for such practices by October 2026.
To ensure that foster youth fully benefit from their family network, the department should, by October 2026, include provisions for continued engagement with siblings and sibling relationship development and maintenance in its five‑year System Improvement Plan for 2024 through 2029.
To ensure that it provides a safe space for foster children and youth in the new transitional shelter, the department should, by October 2026, develop policies and processes for tracking and minimizing overstays at its transitional shelter. The policies and processes should include a biannual review that analyzes trends and outcomes of strategies the department uses to minimize overstays, including a determination of the effectiveness and appropriateness of each strategy.
To ensure that it identifies and corrects any past deficiencies before it reopens the new transitional shelter, the department should, by October 2026, collaborate with its transitional shelter contractors and implement policies and processes for the quarterly evaluation of transitional center performance, such as reviewing compliance with its operating standards, facility standards, and standards of reporting critical incidents. The policies and processes should include the documentation of corrective actions. The department should also implement procedures for tracking trends in critical incidents at the new facility to ensure that it can address any deficiencies it identifies.
To ensure that department staff receive the required core and continuing training in a timely manner, the department should do the following by October 2026:
- Develop and document a process to track child welfare workers’ and supervisors’ progress in completing all required continuing training and report regularly to department management the training completion records for all staff. This process should include creating periodic reminders for child welfare workers and supervisors to complete annual continuing training.
- Establish processes to hold child welfare workers and supervisors accountable for completing the core training and annual continuing training. For example, the process could incorporate completion of training requirements in staff performance appraisals.
To ensure that it can monitor the timely provision of services, the department should, by October 2026, make sure that all contracts include the RBA measures, such as timeliness performance metrics for service provision.
We conducted this performance audit in accordance with generally accepted government auditing standards and under the authority vested in the California State Auditor by Government Code section 8543 et seq. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on the audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Respectfully submitted,
GRANT PARKS
California State Auditor
September 23, 2025
Staff:
Kris D. Patel, Audit Principal
Ani Apyan, MPP, Senior Auditor
Shawn Butler
Ralph Flynn
Alexis Hankins
Kaleb Knoblauch
Annie Lloyd
Data Analytics:
R. Wade Fry, MPA
Sarah Rachael Black, MBA, CISA
Lily Nuñez, MPP
Legal Counsel:
Ethan Turner
Appendices
- Appendix A—The Department Did Not Timely Initiate or Close Investigations of All Referrals
- Appendix B—The Department Generally Adhered to Its Caseload Guidelines for the Family Maintenance and Family Reunification Programs
- Appendix C—Scope and Methodology
Appendix A
The Department Did Not Timely Initiate or Close Investigations of All Referrals
State law requires the department to operate a 24‑hour emergency hotline to receive and respond to allegations of child abuse and neglect. The department must initiate an immediate (within 24 hours) in‑person investigation for a youth reported to be in imminent danger or a non‑immediate (within 10 days) in‑person investigation when a youth is not in imminent danger but there is a risk for their safety if the situation is not stabilized at home.
Further, the department should close investigations of referrals within 30 days of completing the first in‑person contact with the youth. However, the department did not always initiate investigations of referrals or complete investigations within the required time frames. Table A provides a breakdown by fiscal year of associated statistics.
Appendix B
The Department Generally Adhered to Its Caseload Guidelines for the Family Maintenance and Family Reunification Programs
In an effort to reduce case assignments and effectively monitor caseload sizes to promote quality and effective service delivery, the department and the union entered into an agreement in 2015 that established caseload guidelines for staff who are assigned cases in certain programs as their primary assignment, including the family maintenance and family reunification programs. The assistant agency director explained that staff with primary assignments to the family maintenance program should only maintain 28 total cases on any given day, whereas staff with primary assignments to the family reunification program should only maintain 19 total cases each day. The total number of cases includes new cases assigned to staff each day, in addition to ongoing caseload the staff carried over from the prior day.
To assess the department’s adherence to these guidelines, we obtained data from the department for fiscal years 2019–20 through 2024–25. We identified the total number of family maintenance and family reunification cases, respectively, assigned to each staff on each day during the audit period. We aggregated the number of days that individual staff had daily caseloads exceeding 28 and 19 cases, respectively, for the two programs. For example, if two staff in the family maintenance program each had a total caseload of more than 28 on a given day, we identified that as two staff‑days with caseloads exceeding 28 cases. As shown in Table B.1 and Table B.2, we found that the department generally adhered to the caseload guidelines when assigning cases for the family maintenance and family reunification programs. With respect to the family maintenance program, the most notable exception is for fiscal year 2022–23 when 17 percent of the department’s daily staff assignments exceeded the guideline of 28 total cases each day. In contrast, the department only exceeded the guideline of 19 total cases each day for the family reunification program for 2 percent of all staff‑day assignments during fiscal year 2022–23.
Appendix C
Scope and Methodology
The Audit Committee directed the California State Auditor to conduct an audit of the Alameda County Department of Children and Family Services regarding its role in ensuring the health and safety of youth in the foster care system, the department’s process and efforts to ensure that foster youth and children have timely access to services, and the department’s efforts to ensure timely and adequate investigation of child abuse and neglect reports. Table C lists the objectives that the Audit Committee approved and the methods we used to address them. Unless otherwise stated in the table or elsewhere in the report, statements and conclusions about items selected for review should not be projected to the population.
Assessment of Data Reliability
The U.S. Government Accountability Office, whose standards we are statutorily obligated to follow, requires us to assess the sufficiency and appropriateness of computer‑processed information we use to support our findings, conclusions, or recommendations. In performing this audit, we relied on electronic data files that we obtained from Alameda County related to referrals, cases, out‑of‑home placements, and child worker caseloads. To evaluate these data, we reviewed information about the data, interviewed staff knowledgeable about the data, conducted electronic testing of key data elements, and conducted limited accuracy testing. As a result of our work, we found that the data was of undetermined reliability. Although we recognize that the reliability of the data may affect the precision of the numbers we present, there is sufficient evidence in total to support our audit findings, conclusions, and recommendations.
Response
Alameda County Social Services Agency, Department of Children and Family Services
August 29, 2025
Grant Parks
California State Auditor
621 Capitol Mall, Suite 1200
Sacramento, California 95814
RE: Response to Draft Report No. 2024-108
Dear Mr. Parks:
The Alameda County Social Services Agency, Department of Children and Family Services (“Department”) has reviewed the findings, conclusions, and recommendations presented in Report No. 2024-108 (“Report”).
① The Department intends to take appropriate action in collaboration with its interagency partners and contractors to implement the recommendations. The Department appreciates that the Report notes that delays, both in investigations and in ensuring youth receive the services needed, are often not within the Department’s control. The Report also indicates that the Department is proactively making efforts to address its high vacancy rates and enhancing its family finding and engagement efforts.
The Department is dedicated to continuous improvement and looks forward to sharing its implementation progress, including identifying any impediments and barriers, in the upcoming review.
Sincerely,
Michelle Love
Assistant Agency Director
Department of Children and Family Services
Alameda County Social Services Agency
cc: Andrea Ford, Director, Alameda County Social Services Agency
Susan Muranishi, County Administrator, County Administrator’s Office
Donna Ziegler, County Counsel, Office of the County Counsel
Comment
California State Auditor’s Comment on the Response From the Alameda County Social Services Agency, Department of Children and Family Services
To provide clarity and perspective, we are commenting on the response to our audit report from the department. The number below corresponds with the number we have placed in the margin of the department’s response.
① The department’s response overstates and generalizes our report’s observations and conclusions with respect to timeliness when conducting investigations and providing services to foster youth. Our report distinguishes between the timely start of investigations—which as we describe were often outside the department’s control—versus how long it took the department to complete investigations once initiated. As we state, the department’s case files for seven of the 10 late investigations that we reviewed did not provide any details explaining why the investigations were not completed timely following their initiation. For example, our audit describes examples of allegations, including four that posed immediate risk of abuse, neglect, or exploitation of the youth, that were not closed until as many as 476 days after the 30‑day deadline required by CDSS. Similarly, the department’s records did not explain why important services—such as health and dental services—for foster youth were late for 23 of the 27 support cases we reviewed that had documented delays. For example, as we show in Table 3, 13 cases with dental services that we reviewed were delayed by an average of 318 days after the required 30 days of removal from the home.
Footnotes
- State law defines foster youth as children or nonminor dependents who are dependents or wards of the juvenile court or who are at imminent risk of entering foster care. For the purposes of our report, we reviewed only the population under the age of 18 and we refer to this population as youth. ↩︎
- The number presented is based on Berkeley California Child Welfare Indicators Project data from July 2024. ↩︎
- Since July 2016, all 58 counties in California are using the CDSS-prescribed SDM tools to help assess the risk and safety of vulnerable youth. ↩︎
- A placement episode is the period from a youth’s first removal from the home to the youth’s final and permanent placement. ↩︎
- An All County Letter is a notice from CDSS to all county departments of social services that contains instructions and information for the departments to follow. ↩︎
- In assessing the department’s performance, we did not include those referrals that the department had not initiated as of the beginning of April 2025, when we obtained the data. ↩︎
- Edwards and Wildeman, Characteristics of the Front‑Line Child Welfare Workforce,” Children and Youth Services Review, 2018. ↩︎
- The union agreement states that child welfare workers who exceed the caseload size standards for their respective assigned program shall receive a premium payment for each pay period their caseload exceeds such standards. ↩︎
- The CHDP program ended on July 1, 2024, although its services continue under Medi‑Cal. As a shorthand, department staff still refer to health and dental checkup services as CHDP services in case plans and in contact notes. ↩︎
- Relatives can include grandparents, adult siblings, and other adults related by blood, adoption, or affinity within the fifth degree of kinship or by marriage (even if ended by death or dissolution). For example, the relationship between a youth and their first cousin is within the fifth degree of kinship because five or fewer generations separate them. ↩︎
- We selected 10 cases for review. In four of these cases, the department’s investigation took place before our audit period because the youth had already been in the foster care system for more than two years. In one other case, a child and family service agency in a different county conducted the investigation because the case was within the other county’s jurisdiction at the time. Further, the department lacked processes to ensure that staff included the required information in court reports. As a result, we chose not to increase our selection of cases and instead chose to review the remaining five cases to assess the department’s initial family finding efforts. ↩︎
- The California Child Welfare Indicators Project is a collaboration between the University of California, Berkeley and CDSS. The project is housed in the School of Social Welfare and provides access to critical outcome information on California’s child welfare system to agency staff, policymakers, researchers, and the public. ↩︎
- Casey Family Programs is a nonprofit organization whose mission is to provide, improve, and ultimately prevent the need for foster care. ↩︎
